
Health Information Exchange (HIE): A Primer and Provider Selection Guide
Content
1 Purpose of White Paper
1.1 Purpose
1.2 Executive Summary
1.3 Disclaimers
2 Health Information Exchange
2.1 Modalities of Health Information Exchange
2.2 Types of HIE Entities and Networks
2.3 Prevalence of Health Information Exchange
3 Types of Health Information Exchanges
3.1 Types of Architecture
3.2 Types of Communication Methods
3.3 Types of Data Exchanged
3.4 Types of Services Offered
4 Benefits of HIE
4.1 Better Care Coordination
4.2 Access to Right Information/Right Time
4.3 Fewer Errors and Duplicate Tests and Procedures
4.4 Improved Population Health
4.5 HIE in LTPAC
5 Importance of Governance
5.1 Organizational Principles
5.2 Trust Principles
5.3 Business Principles
5.4 Technical Principles
6 Potential LTPAC Provider Business Models
6.1 CMS Health IT Adoption Incentives Medicare (Medicare and Medicaid)
6.2 State Medicaid Grants
6.3 Potential Affordable Care Act (ACA) Opportunities
6.4 Private Pay
6.5 Standard of Care and Other Payment Sources
6.6 Return on Investment (ROI) of HIE
6.7 ROI to Patients and/or Their Families
6.8 ROI to Payers
6.9 ROI to Care Provider
6.10 Online ROI Calculator
7 Planning for and Selecting Appropriate HIE
7.1 Visioning and Strategic Planning
7.2 Organizational Readiness Assessment
7.3 Operational and Programming Planning
8 Role of System Integrators
8.1 Message-Oriented Integration
8.2 Application-Oriented Integration
8.3 Coordinated-Oriented Integration
8.4 Middleware-Oriented Integration
9 HIE Matrix Components
10 Acknowledgement of Contributors
10.1 Contributing Writers
10.2 Workgroup Members
11 References and Resources
1 Purpose of White Paper
1.1 Purpose
The purpose of this paper is to aid LeadingAge and other aging services organizations in understanding health information exchange (HIE) modalities, the range of HIE entities, and networks serving the market. It includes vendor-sponsored HIE networks, their value-added services, and their benefits. In addition, the white paper will help providers plan for and select an HIE partner. The paper will include a matrix of existing HIEs that will help providers select solutions that best fit their requirements.
This white paper will help providers plan for and select a health information exchange (HIE) partner.
1.2 Executive Summary
The Health Information Exchange (HIE): A Primer and Provider Selection Guide is a white paper intended to help LeadingAge members and other aging services organizations understand the uses and benefits of HIE modalities, the range of HIE entities, and networks serving the market. It covers vendor-sponsored HIE networks, their value-added services, and their benefits.
The white paper is part of an HIE Technology Selection Tool that includes an interactive guide, selection tool and matrix of existing HIEs, and provider case studies to help providers plan for, select, and implement the technology solutions that best fit their requirements.
The white paper explains the different types of HIE entities and networks, including the various types of architecture, communication methods, data exchanged, and services provided. Generally, all serve the same role as “unbiased data trustees” that don’t provide care, but that use advanced technology to deliver on a community’s needs.
Next, the white paper shares the benefits of HIE, including better care coordination, the ability to access the right information at the right time, fewer errors, fewer duplicate tests and procedures, and improved population health. It’s important to note that long-term and post-acute care (LTPAC) providers’ participation in HIE activities lags behind the rest of the healthcare sector. LTPAC providers must fully participate in HIEs to be able to effectively partner with accountable care organizations and participate in other alternative payment models to succeed in monitoring and addressing the health concerns of older adults who need extended or long-term care.
The white paper also covers the importance of HIE governance and the role of system integrators. Potential LTPAC provider business models are included to help organizations learn from others’ experience. A section on planning for and selecting the appropriate HIE speaks to the cybersecurity concerns of HIEs, and it points to the LeadingAge CAST Cybersecurity Resources that can address these concerns.
Lastly, the white paper shares the components of the HIE matrix that is part of the tool, used to help organizations narrow the possible products: Service location, modality of exchange, type of HIE entity, type of data exchanged, services offered, communication method, LTPAC electronic health record supported, consent policies, company experience, contact information, and strengths.
CAST offers seven additional online technology selection tools, complete with hands-on resources. Each portfolio includes a white paper, selection matrix, online selection tool, and provider case studies. All help you to understand, plan for, select, implement, and adopt the appropriate technology while advocating for innovative care models.
1.3 Disclaimers
This information is meant to assist in understanding HIEs, but it cannot possibly include every exchange option that is available. Exchanges mentioned in this report are only illustrative examples and have not been tested or independently evaluated or endorsed by LeadingAge or LeadingAge CAST. Please use this information as a general guideline in understanding HIE functionalities. Where appropriate, we identified provider case studies.
2 Health Information Exchange
Health information exchanges, or HIEs, are organizations or frameworks that allow for the secure and timely exchange of protected health information (PHI) between providers, caregivers, health insurers, and other organizations that have an interest in a patient’s care. These exchanges can be largely technical and can be a multi-stakeholder partnership where otherwise competitive organizations can collaborate on use cases that create better value for participating entities and better outcomes.
HIEs are “unbiased data trustees” that don’t provide care, but that use advanced technology to deliver on a community’s needs.
There are many different varieties of HIE: regional, statewide, nationwide, and vendor to vendor are all examples of the different flavors of HIE entities that now exist in the United States. Even though there are many different types, they generally all serve the same role as “unbiased data trustees” that don’t provide care, but that use advanced technology to deliver on a community’s needs.1
2.1 Modalities of Health Information Exchange
HIE has evolved over the past 20 years, creating three core types of HIE modalities:
- Directed Exchange (Push).
- Query-Based (Pull).
- Consumer Mediated.2
These different types of exchange drive different use cases. We will examine the main use cases supported by these different types of exchange and the prevalence of HIE in the country.
2.1.1 Direct Push Exchange
Push exchange is used today to send alerts and individual pieces of clinical data that are delivered automatically to a provider without much special effort. This type of push exchange has enabled use cases like encounter alerts, lab results delivery, and delivery of data to public health registries. Push is also used to enable the directed secure messaging between two providers, much like e-mail. This type of push exchange supports use cases like referrals, care coordination, and transitions of care.
Push-based exchange, especially encounter notification, is especially important in the context of value-based payment models.
While providers have always had a clinical interest in knowing about (and, in turn, some care coordination responsibilities with regards to) patient encounters and care outside of their practice or facility, new models are shifting financial incentives and risk to providers, making ‘patient panel intelligence’ increasingly central to financial success. Infrastructures that support notifications also have the potential to better engage patients, families, and caregivers.3
Secure messaging was a critical component of the Meaningful Use incentive program. It has been widely implemented inside the electronic health record (EHR) for most providers, particularly those who were eligible for such incentives, like hospitals and physician offices.
That said, Meaningful Use often did not include long-term care (LTC) providers, so the penetration of Direct Secure Messaging within LTC EHRs may not be as widespread. The primary use case for Direct messaging is to allow providers to send secure e-mail messages between providers in an encrypted fashion with PHI sent inside the message. The option of web-based Direct messaging is available to LTPAC and home care organizations to support secure messaging with healthcare providers, especially in support of information exchange to support hospital discharge. The trade organization DirectTrust manages the relationships between different secure e-mail providers such that messaging can occur across different domains “without requiring providers to manage the use of different portals or domain-specific solutions.”4
2.1.2 Query-Based/ Pull Exchange
Query-based exchange enables providers to find and “pull” information on a patient from other providers through a health information exchange. Generally, this happens when not much is known about a patient or when the provider expects to find new information in patient records kept by other providers.
Query-based exchange was one of the original HIE use cases, mostly through the use of web-based portals where providers would enter demographic information and view a consolidated health record. Advancements in query-based exchange include single sign-on (one click access to a web-based portal), exchange based on application programming interfaces (API), which give automatic access to health information, and a new standard called Fast Health Information Resource (FHIR), which uses technology to make it easier for a provider to pull health information into an EHR.
To make the HIE query resource valuable, a health information organization (HIO) must serve up the right information, to the right person, at the right time, using the right tools, and at the right moment in the clinical workflow.
- The right information: Is the right information available through the HIO to address a clinical end-user’s treatment or diagnosis needs?
- To the right person: Is a physician, nurse, mid-level, scribe, or other care team member the right person to be interacting with the data?
- In the right way: Clinical Decision Support (CDS ) intervention format: Is the data formatted in a consumable way?
- Through the right channel: Is a web-portal sufficient, or would single-sign on and patient context passing be necessary? To be successful, how tightly tied to an electronic medical record (EMR) or health information system does the query process need to be?
- At the right time in workflow: Is the data helpful in advance of an encounter (planned), at the time of patient arrival, at initial history and physical, or at some other point in the course of care?5
- To make the HIE query resource valuable, an HIO must serve up the right information, to the right person, at the right time, using the right tools, at the right moment.
2.1.3 Consumer Mediated Exchange
According to HealthIT.gov: “Consumer Mediated Exchange gives patients the ability to aggregate and manage their health information on the internet. When in control of their own health information, patients can help transfer information between providers, correct inaccurate demographic, medical, or billing information, and track and monitor their own health.”6
The idea of consumer mediated health information exchange has historically been very hard to implement. Most HIE organizations interact with patients just through consent workflows, allowing patients to decide what types of electronic exchange they consent to. That said, recent improvements in technology have created more capability for patients to control their own data.
Two of the most notable cases of consumer-mediated exchange are the “Blue Button” initiative, which allows Medicare patients to have simple access to their Medicare records through the electronic method of their own choosing7, and the recent integration of Apple’s Health application into the EHRs of many major hospital and outpatient laboratory systems.8
These are the three main types of exchange that are most prevalent in production today. These types of exchanges can be seen at many different levels of geography and business.
2.2 Types of HIE Entities and Networks
In this section, we will describe the many different types of HIE entities and networks that exist today throughout the country. Many of these exchanges exist to serve specific use cases and work together to ensure that all use cases are manageable in a community. The landscape of HIE networks is always changing, and the legal requirements of the 21st Century Cures Act of 2016 could have a significant impact on the landscape in the coming years.
The landscape of HIE networks is always changing, and the 21st Century Cures Act of 2016 could have a significant impact in the coming years.
2.2.1 National HIE Networks
A key component of the 21st Century Cures Act of 2016 that could be especially impactful is the Trusted Exchange Framework and Common Agreement (TEFCA). It is expected to become finalized in 2019 and implemented in 2020 and beyond. This regulation seeks to better define the landscape of national HIE networks and how they operate with each other. In this section of the paper, we will examine the large national HIE networks that exist today. If you are interested in learning more about the evolving TEFCA, please consult with the Office of the National Coordinator for Health IT or The Sequoia Project.
2.2.1.1 Carequality
Carequality is “a national-level, consensus-built, common interoperability framework to enable exchange between and among health data sharing networks.”9 The network’s participants are a cross-section of the HIE industry, including major EHR vendors, statewide and regional health information exchanges, patient-facing health IT technologies, health plans, and others.
While Carequality does not provide any technical capabilities, it creates the technical and policy framework that allows different organizations to follow the same rules when they exchange with each other. As an example, General Hospital, utilizing their EHR vendor, could use query-based exchange to ask City Hospital, which uses a different EHR vendor, for the record of a common patient.
Carequality sets the policies through which the hospitals agree to that query-based exchange and the technological strategy over which the hospitals do the actual exchange. Carequality does not provide any of the actual software or hardware the data travels through to get from City to General. For more information, see Carequality.org.
2.2.1.2 eHealthExchange
“Active in all 50 states, the eHealth Exchange is the largest query-based, health information network in the country. It is the principal network that connects federal agencies and non-federal organizations, allowing them to work together to improve patient care and public health.”10 The eHealthExchange is the most common method for organizations to perform query-based health information exchange with federal agencies like the Veterans Administration (VA), Department of Defense Military Health, and the Social Security Administration.
eHealthExchange provides routing technology and will soon provide a hub11 through which one provider could perform query-based exchange with another provider anywhere in the country. In the above example of the exchange between General Hospital and City Hospital, eHealthExchange could provide the technology over which the record is exchanged. For more information, please see eHealth Exchange.org.
Carequality and the eHealth Exchange operate under the same parent company, The Sequoia Project. The technical operations manuals of both organizations use the same widely adopted technical standards for query-based exchange. Integrating the Healthcare Enterprise released these standards, which most EHR vendors and all Certified eHealth Technology can easily support.
2.2.1.3 Patient Centered Data Home
In the previous two examples of national HIE networks, the primary modality of exchange is query-based or “pull” exchange. In contrast, the Civitas Networks for Health (formerly known as the Strategic Health Information Exchange Collaborative (SHIEC)) Patient Centered Data Home (PCDH) network is a national network that largely supports the “push” modality of exchange. This approach ensures that a medical record follows a patient to their “home” HIE network and ultimately to their provider.
PCDH uses a large network of over 42 state and regional HIEs. It is a vehicle to close the loop on care when a patient is seen outside their normal care area, through existing HIE technology that preserves local governance.12 The PCDH network provides both the policy and technical framework through which health information can be exchanged. While it does not create or operate technology itself, it leverages its member HIE technology to move messages throughout the country.
In this example, a patient is seen for care at the out-of-state Academic Hospital. Through the PCDH network, the details of that encounter are routed to the state HIE that Academic Hospital participates in. That out-of-state HIE automatically finds the HIE in the patient’s home state. The encounter details are then routed automatically to the patient’s home HIE, which delivers the information automatically to the patient’s provider(s). Learn more.
2.2.2 State and Regional HIEs
The genesis of most state and regional HIEs came from the 2009 HITECH Act. As part of the American Recovery and Reinvestment Act of 2009, the act allocated more than $500 million to 56 states and territories to create “critical health technology infrastructures” meant to modernize and make electronic the American healthcare system. These individual statewide or regional health information exchanges facilitate interoperability across the entire healthcare system. They also support community use cases in accordance with state policies and regional laws.
State and regional HIE networks are often not-for-profits that collaborate with local stakeholder organizations.
These HIE networks are often not-for-profits that collaborate with local stakeholder organizations to form a governance and technology framework through which PHI can move between a patient’s care team members. A typical state or regional HIE supports both the “push” and “pull” modalities of exchange, using the same technical standards as the national networks.
State and regional HIEs tend to not only provide tools and services to traditional healthcare institutions like hospitals, practices, payors, long-term and post-acute care providers, and public health organizations. They also have evolved to serve local social service organizations like those that address food, housing, and other environmental issues. Several local HIEs are participating in the Accountable Health Communities program from the Centers for Medicare & Medicaid Services (CMS), which supports “local communities in addressing the health-related social needs of Medicare and Medicaid beneficiaries by bridging the gap between clinical and community service providers.”13
Civitas Networks for Health is a national collaborative comprised of member organizations working to use health information exchange, health data, and multi-stakeholder, cross-sector approaches to improve health. We were previously known as the Strategic Health Information Exchange Collaborative and the Network for Regional Healthcare Improvement. We represent more than 150 local health innovators from across the US, moving data to improve health outcomes for more than 95% of the U.S. population. Learn more about Civitas Networks for Health.
2.2.3 Other Types of Networks
There are other types of networks that are considered health information exchanges but tend to operate between vendors or within the walls of a single vendor. Here, learn more about two of the most common vendor-led networks.
2.2.3.1 EPIC CareEverywhere
Through the Epic CareEverywhere platform, customers of the Epic Electronic Health Record system can exchange data with each other and with external parties. Using the same query-based technology standards described above, a patient’s record freely moves between two different organizations and is well-integrated into the Epic platform.
The CareEverywhere platform can also be integrated with third parties like state and regional HIEs, and it has integrated with the Carequality network. This allows Epic customers to exchange data between Epic facilities and to the outside world. More than 100 million documents are exchanged each month through CareEverywhere.14
2.2.3.2 CommonWell Health Alliance
The CommonWell Health Alliance is an independent alliance of major EHR vendors to create and promote interoperability efforts between their customers. It has since expanded to “a diverse mix of member companies, ranging from health care organizations and not-for-profits to EHR companies and data exchange vendors.”15 Most of CommonWell’s utilization supports query-based document exchange between provider sites that use vendors that are CommonWell members.
In 2018, CommonWell joined Carequality so that CommonWell network members could implement technology solutions that could interoperate with Carequality members.
Provider organizations are using HIE significantly more since the HITECH Act was passed.
2.3 Prevalence of Health Information Exchange
An organization can participate in health information exchange through a number of different methods. It is a complicated environment, but provider organizations are using HIE significantly more since the HITECH Act was passed.
2.3.1 Aging Service Organizations
As federal money poured in to get hospitals and providers to become “meaningful users” of health information technology, much of that money was not directed at aging service organizations. This is often described as a missed opportunity, because “patients who are aged 65 and older will frequent healthcare facilities roughly 3 to 4 times more often than those under 65.”16
Over time, more aging service providers have adopted EHRs, but there is much work to be done to integrate those providers with HIEs. Where these providers have integrated with an HIE, they have done so to support transitions of care, encounter notifications, discharge planning between hospitals and skilled nursing, and tracking patients who bounce in and out of rehabilitation stays.
Over time, more aging service providers have adopted EHRs, but there is much work to be done to integrate those providers with HIEs.
Dr. Eugene Heslin from the New York eHealth Collaborative said, “You’re going to see patients accessing the healthcare system 12 to 15 times per year among the baby boomer population…. This high number of annual patient encounters presents an ideal opportunity to demonstrate how HIE use can allow for faster patient care delivery, cost savings, reductions in duplicate or redundant testing, and more accurate diagnosis and treatment. Regardless of where these patient encounters occur, HIE use lets different providers at healthcare facilities across state lines obtain patient information for efficient, cost-effective, and well-informed care delivery.” 17
A majority of hospitals and acute care providers are participating in at least one, and in many cases multiple types, of HIE organizations.
2.3.2 Hospitals and Acute Care Providers
A majority of hospitals and acute care providers are participating in at least one, and in many cases multiple types, of the HIE organizations described above. Hospitals are likely to be automatically participating in national networks like CommonWell, Epic CareEverywhere, or Carequality through their EHR vendor’s default integration. Those implementations will provide access to some query-based document exchange. Often hospitals are also connecting to local state and regional HIEs to gain access to different information types and to support use cases important to their communities.
Typical use cases implemented at hospitals include query-based exchange to learn information about patients for which they have no prior record; push based exchange, through state and regional HIE integrations, to notify providers in the community of hospital visits as they happen; and the delivery of clinical data from a hospitalization to the next provider through a transitions of care workflow.
According to data from 2017, “Nearly seven in 10 hospitals (69%) participated in a state, regional, and/or local HIO. While six in 10 small hospitals participated in a state, local, or regional HIO, about three-quarters of medium to large hospitals did so.”18
2.3.3 Payers
Payer participation in HIE has also grown overtime with more than half of state and regional HIEs reporting payer participation and almost 38% of state and regional HIEs having at least four participating payers in the HIE. Traditionally the implementation of value-based use cases has driven payer participation in HIE. In many locations, Medicaid managed care organizations will use HIE services to jump start their interoperability efforts.
In the future, payer participation is likely to grow, as proposed “information blocking” regulations from the Office of the National Coordinator will require payers to respond to requests for health information from other payers and providers.19
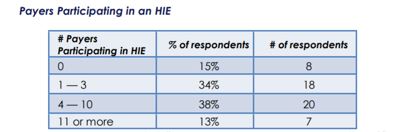
Fiqure 2. HIEs were asked, “How many payers participate in your exchane?”20
3 Types of Health Information Exchanges
3.1 Types of Architecture
3.1.1 Centralized Model
This model of HIE means that all data is stored centrally, in one single or consolidated repository, and each participant’s data is regularly submitted directly to this entity where it is then stored and accessed. In this model, the HIE holds and “stewards” the data . This is most often the product of an existing organizational structure.
The centralized data repository is often favored for purposes of population health management or analytics. A core challenge is patient/data matching. There are no shared identifiers, as it is all within one system.
3.1.2 Federated Model
A federated model of HIE is a decentralized model where data is held at the participant source and the participant is a member of the HIE, agreeing to send the information to other members/participants. This type of model requires a record lookup or locator service, so that when one participant queries (looks for) records on a patient, the system retrieves them. In this model, there is no data held in the HIE itself.
A federated model also doesn’t require a single system. Each participant can submit their data from their prospective systems. That way, if one system goes down or has a technical issue, it doesn’t impact the entire HIE. This model is often favored for activities that require pushing data, and regional or statewide health information organizations most often adopt it.
3.1.3 Hybrid
A hybrid model combines the features of a centralized and federated model. It includes both a central data repository and a record locator service, connecting both services.
3.2 Types of Communication Methods
3.2.1 Secured Web Services
This type of communication allows HIE members to exchange patient data through a web application, such as a portal mechanism. Certain key record identifiers or requests for information are stored in the HIE. However, a record locator key is still leveraged to identify, retrieve, and send medical information upon request.
3.2.2 TCP/IP over VPN
This model allows computers to communicate over a secure private network and provides end-to-end connectivity, with specifications on how data should be formatted, addressed, transmitted, routed, and received at the destination. This method is the most-connected, most interoperable way to exchange health data in an HIE.
3.2.3 Secured FTP
This method allows organizations connected to an HIE to send patient data in batches or one at a time. This is not a real time solution. but because it enables sharing of patient data, it meets Meaningful Use electronic data exchange requirements as specified in Stage 1.
3.2.4 Secure E-Mail
The Direct protocol paves the way for scalable and secure health information exchange. It allows users to send and receive authenticated, encrypted health information between known and trusted recipients, regardless of the originating application system or platform. Service organizations can also use secure email within their EHR to exchange patient health information with other providers in their network, and outside their network if the outside provider has a Direct email address.
There are a number of ways to exchange patient information securely within networks. Examples include patient portal and the secure email messaging functionality in a certified EHR, following a specific workflow designed to differ from one system to another. Most EHRs have security features that are built in but not always configured or enabled properly. To protect the safety of electronic protected health information, it’s important to ensure the EHR has the safety guards in place.
There are many ways to exchange patient information securely within networks.
3.3 Types of Data Exchanged
3.3.1 Admission, Discharge, Transfer (ADT)
This is the most common type of health data message exchanged. ADTs include information on patient events involving admission, transfer, or discharges from clinical care settings, especially emergency department and inpatient hospital visits. This information alerts the patient’s providers and is helpful in care coordination and care management.21
3.3.2 Demographics
Patient demographics (name, date of birth, sex, preferred language, race, and ethnicity) are part of the Common Clinical Data Set (CCDS) that is used to identify each patient. Demographics are part of the larger standard Continuity of Care Document (CCD) that is used to exchange patient health information.
3.3.3 Care Plan
The care plan as expressed in the Consolidated Clinical Document Architecture (C-CDA) standard does not attempt to represent the longitudinal care plan. Instead, it represents a “snapshot” of a care plan at a single point in time for transmission to other providers and teams to ensure continuity of care.
Care plans provide direction for individualized patient care. A care plan flows from each patient’s unique list of diagnoses and should be organized by the patient’s individual specific needs. The care plan is also intended for use with continuity of care and is used to communicate and organize the actions of a care team (physician, nurse, and other practice staff).
3.3.4 Allergies
A patient’s medication allergies are included in the CCDS exchanged in the CCD to help avoid an adverse reaction with any medications he or she is currently taking.
3.3.5 Medication List (Last Reconciliation and Fill Data)
Medication reconciliation of a patient’s medication list and history is completed at the office visit within the EHR system. It is important for a number of reasons pertaining to patient care, including medication allergies and adverse reactions. Having this information could avoid overprescribing and combat prescription drug abuse.
3.3.6 History and Physical (H&Ps)
History and Physical is a standard template for a patient’s medical history. This often includes patient demographics, chief complaints, history of present illness, past medical history, family history, social history, allergies, medication history, review of systems, and physical examination.
3.3.7 Patient’s Advance Directives
This is the legal document that tells providers about a patient’s wishes for care in the event the patient is not able to communicate them directly, including for end-of-life care. This can include whether to accept or refuse medical care and/or more detailed information or instructions about the use of breathing machines or dialysis, whether or not to resuscitate if a patient’s breathing or heartbeat stops, tube feeding, and organ or tissue donation.
Please note that not all HIEs are able to exchange advance directives; however, some HIEs are facilitating this type of exchange.
3.3.8 Electronic Reporting Immunizations
Immunizations are vital to public health across the United States. Higher immunization rates protect vulnerable children who are too young to be vaccinated and people with chronic diseases who can’t be vaccinated for medical reasons. However, because immunization rates vary from state to state, some communities have experienced preventable disease outbreaks.
Tools provide immunization data that can help family physicians identify populations that may be at risk of vaccine-preventable diseases.
The American Academy of Family Physicians has developed a web-based map that displays immunization rates and exemption laws in all 50 states, D.C., Puerto Rico, the Virgin Islands, and Guam. In addition, the searchable Immunization Information Systems Registry database provides state-by-state regulations for immunization registries across the United States.
These tools provide immunization data that can help family physicians identify populations that may be at risk of vaccine-preventable diseases like measles and pertussis (whooping cough), determine what additional resources and/or programs are needed to increase immunization rates, determine how immunization exemptions affect their state immunization rates, and advocate for stronger immunization legislation in their communities.
While there is still work to be done in terms of exchanging this vital information, some states have already implemented direct connections with their respective HIEs to automatically submit immunization records to the state’s registry.
3.3.9 Problem List
A problem list is a document that states the most important health problems facing a patient, such as nontransitive illnesses or diseases, injuries suffered by the patient, and anything else that has affected the patient or is currently ongoing with the patient. Problem lists facilitate continuity of patient care by providing a comprehensive and accessible list of patient problems in one place. Additionally, problem lists usually identify a timeframe for onset or occurrence of a problem and description of resolution. They are an important communication vehicle used throughout the entire healthcare continuum.
3.3.10 Situation, Background, Assessment, and Recommendations (SBAR)
SBAR is the prevailing framework for handoffs in a healthcare setting between providers and clinical staff used to standardize communication in acute care situations. But it has also been applied in other clinical situations to increase provider communication overall. This framework provides a structure for presenting medical information about a patient in a known and logical sequence, as it is a common language between providers.
3.3.11 Electronic Intervention to Reduce Acute Care Transfers (INTERACT) Admission Form
This electronic form is part of a larger quality improvement initiative aimed to manage acute changes in resident conditions. The goal of the program is to improve care and reduce the frequency of potentially avoidable transfers to the acute setting.
PointClickCare has incorporated the electronic INTERACT (eINTERACT) tool to enable patient tracking and ultimately reduce readmission rates and unnecessary transfers. eINTERACT allows for clinical alerting, clinical documentation, quality improvement tracking, and other functionality. The eINTERACT transfer form is used when a resident is being transferred to a hospital and is triggered when the nurse discharges or transfers the resident into an acute care hospital. There are several other modules available through eINTERACT.
3.3.12 Laboratory Results
The industry standard for exchanging laboratory orders and results is via Logical Observation Identifiers Names and Codes (LOINC). LOINC is a common set of identifiers, names, and codes for exchanging health measurements, observations, and documents. LOINC includes specimen-specific laboratory tests as well as clinical or non-specimen test results and observations of a patient. LOINC aims to facilitate the collection and exchange of results and identify the test result or clinical observation. LOINC is used to identify health measurements, observations, and documents.
3.3.13 Image Exchange
Image Exchange allows for a patient’s diagnostic imaging results to be exchanged among a patient’s care team. Image Exchange services have proven useful in reducing unnecessary testing and beneficial in telemedicine and remote monitoring.
3.3.14 Public Health Reporting
Public health agencies receive data for reporting and registries from screening and treatment services, laboratories, pharmacies, various medical/clinical providers, and more. Public health connectivity to an HIE can add to the robustness and timeliness of the data they receive.
3.3.15 Discharge Summary
This information can be shared under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) Privacy Rule. Elements that comprise a discharge summary within a CCD include patient name, date of birth, discharge date, admission and discharge diagnoses, procedures, physician information, lab results, procedures, follow-up testing, discharge medication list, results and findings, and discharge plan of care. Other elements that may also be included are problem list, resolved hospital problems, past medical history, summary of hospital course, and weight and vital signs.
3.3.16 Functional Assessment
Functional reporting gathers data on beneficiaries’ functional limitations during the therapy episode of care as reported by physical therapy, occupational therapy, and speech language pathology therapy providers and practitioners.
3.3.17 Cognitive Assessment
This testing checks for problems with cognition, including memory, thinking, language, judgment, and learning. There are several common cognitive assessments, all lasting a few minutes testing a patient’s ability to memorize and recall various elements.
3.3.18 Physician Orders for Life-Sustaining Treatment (POLST)
POLST is a set of medical orders, similar to a do-not-resuscitate order, intended for patients who are considered to be at risk for a life-threatening clinical event. It is designed to support patients in care transitions between facilities, or between the community and a facility. The POLST form is a recognizable and standard medical order.
Electronic exchange of POLST can allow healthcare providers, including Emergency Medical Services (EMS), to access this information at all times.
POLST improves the quality of care by providing a standard system for identifying patient wishes regarding medical treatment through a portable medical order. It is designed to support and supplement advance directives. The electronic exchange of POLST can allow healthcare providers, including Emergency Medical Services (EMS), to access these forms and information at all sites and all times.
3.4 Types of Services Offered
HIEs play an important role in giving providers access to patient information to support care delivery and care coordination. HIEs commonly offer core services and tools that help members/participants improve their quality of patient care.
HIEs play an important role in giving providers access to patient information to support care delivery and care coordination.
3.4.1 Consolidated Clinical Summary Record Exchange
A Continuity of Care Document (CCD) is a human-readable, longitudinal summary of pertinent
demographic, clinical, and administrative data for a specific patient. The CCD is one of the document types based on the HL7 Clinical Document Architecture (CDA), an industry-accepted standard governed by the HL7 organization.
From a clinical standpoint, the information presented by a CCD intends to give care team members a snapshot of a patient’s medical history. It conveys data in sections such as Encounters, Diagnoses, Medications, Allergies, Vital Signs, etc. The Office of the National Coordinator (ONC) Meaningful Use Stage 2 program required that CCD documents be capable of supporting all data elements from the Common Clinical Data Set (CCDS). As a result, this has become the gold standard for data sections within the CCDs exchanged by ONC-certified EHR vendors.
The implementation of the CCD standard can vary across systems. But one of the CCD’s primary purposes is to exchange clinical data between care settings to support continuity of care for patients. HIEs facilitate the electronic exchange of clinical and administrative data across the boundaries of authorized healthcare providers and facilities by providing an electronic mechanism to do so. As integrators and data aggregators, HIEs rely on the CCD standard for data exchange.
3.4.2 Consolidated Summary EHR Record from Multiple Providers
Some HIEs create a single person-centered consolidated EHR summary record from multiple summary records generated by EHR systems of providers with whom the patient interacted. These summaries come in the form of Consolidated Clinical Document Architecture (C-CDA), which is usually used in creating summary records exchanged.
Consolidation aims to provide comprehensive data about the patient while reducing redundancies through de-duplication of data.
Providers may include hospitals the patient visited, physicians and specialists that have recently seen the patient, pharmacies where the patient filled prescriptions, etc. This consolidation aims to provide comprehensive data about the patient while reducing redundancies through de-duplication of data. It also reconciles discrepancies and even contradictions in data.
3.4.3 Patient Centered Data Home (Regional and National Networks Only)
Patient Centered Data Home (PCDH), set forth by Civitas Networks for Health (formerly known as Strategic Health Information Exchange Collaborative (SHIEC)), has been implemented to enable the exchange of patient data between community HIEs. Through this model, patients are assigned a “home” HIE, and providers within that HIE are notified when an event takes place for that patient within the other connected HIEs.
That patient’s “home” providers then can access relevant clinical data for the patient’s events that occurred outside of the “home” HIE. The main standards used for PCDH’s data exchange model include ADT push, CCD push, and CCD query in a way that is compliant with the standards of Integrating the Healthcare Enterprise (IHE) and Cross-Enterprise Document Sharing (XDS) standards known as XCA. Currently, 42 community/regional HIEs make up PCDH.
3.4.4 Health Information Service Provider (HISP)
Many HIEs have health information service provider (HISP) responsibilities such as issuing Direct addresses and providing the mechanism to deliver messages securely via Direct. An HIE with a certified HISP acts like the postal service. It provides the transport and security mechanisms to move communications from one HISP to another.
3.4.5 Electronic Authentication as Shared Service
HIEs provide user identity and access management services that establish identity proofing and authentication controls. The Office of the National Coordinator (ONC) has recently called states to develop effective and efficient identity management solutions for providers and consumers in the value-based payment landscape. Leveraging HIEs is a way to streamline identity management solutions.
ONC has recently called states to develop identity management solutions for providers and consumers.
Authentication is a critical function of HIEs, as it sets the foundation for appropriate access and can have a negative downstream effect if not implemented correctly. Similar to online banking solutions, HIEs typically have applications that can accept credentials and control user privileges based on roles or level of access.
Identity proofing is the process of validating information that has been collected about a user who holds credentials in order to verify the user’s identity. The identity proofing process helps to establish a trusted relationship for the purpose of electronic authentication. To have confidence in user identity, the electronic authentication process requests information from users each time they log into the system.
HIEs and healthcare organizations complying with the HIPAA Security Rule and national recommendations set forth by ONC and other standards organizations commonly leverage technical guidelines set forth by the National Institute of Standards and Technology around implementing electronic authentication.
3.4.6 Patient Matching (Master Patient Index – MPI)
The ability to locate and link patient records across disparate data sources is a foundational function of HIEs. Since HIEs consist of multiple data sources and high volumes of patient records, and since the U.S. does not yet have standard unique patient identifier, master patient indexes (MPIs) are one of the key components or services necessary for data exchange within an HIE infrastructure.
HIEs provide a unified mechanism to check if data from different sources belong to the same patient, in order to craft a complete and accurate record of the patient’s medical history or care summary. A variety of different approaches exists for patient matching. Approaches include unique patient identifiers like demographics, patient biometrics, or using an algorithm to match records together.
There are pros and cons to these approaches. However, data exchange initiatives have leaned toward an algorithmic-based model for matching patients across systems. HIEs often have stewardship over patient matching, as manual intervention may be required when a match cannot be established. Data governance plans have been implemented by HIEs to determine how issues around patient matching should be handled.
3.4.7 Provider Directory
Provider directories support the querying and sending of up-to-date provider and health organization information. When provided as a service by an HIE, a provider directory contains information such as provider demographics, address, credentials, specialty information, provider National Provider Identifier, state license number, and language(s) supported., In some HIEs, a directory also provides a destination address for a Direct messaging service. In addition, a directory may contain information on provider relationships to HIEs, other organizations and providers, care delivery networks, hospitals, and other practice groups.
To be listed in a provider directory, an HIE participant may send a minimum set of data elements to the HIE that will populate a record with provider and network information.8 In other cases, a provider or organization can add, update, or search a record at any time using a web-based login. Depending on the HIE, this data can then be shared through a variety of different standards, including a web-based service, an extracted file, and/or a manual entry into an EHR.
Provider directories can be an instrumental service in value-based payments.
Provider directories can be an instrumental service in value-based payments by maintaining information needed for both providers and payers, as a tool for quality measurement and a tool to provide better care coordination.7
In specific use cases, this service could help to develop better transitions of care by providing accessible contact information for a care team member. As health systems continue to use other technology-based care, a directory can provide information on telemedicine networks and a physician’s electronic capabilities. Having this information accessible in real-time through an HIE to a consumer can lead to many important use cases where this information adds value to the consumer’s daily workflow.
3.4.8 Consent Management
Consent management is a key operational component of HIEs. HIEs facilitate health information sharing in accordance with patient consent decisions through the electronic consent management function. Consent decisions made by patients influence different factors depending on the HIE, such as release of health information, circumstances for release of health information, and authorized access of a patient’s health information. Furthermore, consent models offered by providers and HIEs may be influenced by federal and state laws, HIE policy, stakeholder input, etc.
Consent models implemented at the state level are no consent, opt-in, opt-out, and a hybrid consent model. States with no consent policies do not require express patient consent for the exchange of health information. Opt-in consent models allow for patient choice in the selection of providers who can access their health information via queries to the HIE. Opt-out consent models allow for patients to opt out of the HIE’s provider query function and prevent access to their health information.
There are varying degrees of the HIE’s role in the consent process.
HIEs may also combine opt-in and opt-out policies depending on the type of health information being accessed. For states with opt-in and opt-out consent models, a patient can select different consent options or values that impact data exchange in an HIE environment.
There are varying degrees of the HIE’s role in the consent process, from providing the infrastructure supporting consent policies and procedures to authentication of eligible providers sending consent values collected from patients. On a fundamental level, HIEs support access to patient records through consent management functions based on HIE and state-specific standards and policies.
3.4.9 Proactive Alerts/Push Notifications
At the cornerstone of health IT and HIE lie Admission, Discharge, or Transfer (ADT) notifications, which provide solutions to many of the complex challenges improving patient care coordination. ADT alerts enable EHRs and HIEs to communicate changes to demographic information (name, insurance, attending physician, next of kin) and changes in status when a patient has been admitted or discharged from the hospital or has been transferred to a different medical facility.
At the time of an event, information is sent from the participant’s EHR system to the HIE, generating an ADT alert that is sent along to a patient’s care team. These notifications occur immediately, allowing medical providers and care teams the opportunity to determine appropriate intervention and follow-up to support the patient with post-discharge care needs.
HIEs vary widely across the nation and provide a variety of services to their participants. Notifications can be sent to a wide variety of organizations supporting the patient. They can be integrated into an EHR system or delivered via secure messaging to providers who subscribe to the HIE’s services.
Additional value-added services will vary by HIE and may include event-based alerts (such as admittance to skilled nursing facilities, incarceration or release from jail, and patient expiration), consent alerts, and other critical event notifications that can be customized to support clinical or population-based analytics, quality assurance activities, and reporting.
3.4.10 Referral Services
Closing the referral loop involves exchanging patient information between two providers. The referring provider receives a report from the receiving provider after the patient’s visit is completed. The practice of closing the referral loop is most common between primary care providers and specialists. Historically, it has taken place via phone, fax, and in person.
The Centers for Medicare & Medicaid Services has prioritized closed loop referrals. CMS adopted specific quality measures that seek to improve care coordination by closing the referral loop, using electronic processes.
HIEs can help provide the infrastructure or services that providers need to send and receive patients’ specialist reports and clinical information. Some HIEs may partner and connect with referral management solutions to give their participants an automated and electronic closed loop referral workflow. Alternatively, providers can use an HIE’s Direct secure messaging services to send referral reports.
3.4.11 Patient Access/Portal
Patient portals are a patient’s gateway to their own electronic health information. They can better engage patients in their own health care. Functions such as medication refill requests, secure messaging with providers, and scheduling are other benefits of a patient portal. A patient can use an HIE’s patient portal to see all of their records from disparate data sources, just as a provider can view a patient’s complete records.
A patient can use an HIE’s patient portal to see all of their records from disparate data sources.
While many EHR vendors offer patient portal solutions, an HIE-tethered portal includes patient data throughout the HIE. HIEs can integrate with many systems and aggregate data from multiple sources, which can help build a patient portal as a service to members/participants. HIEs have offered patient portal solutions to support participating providers with Meaningful Use requirements and to encourage patient engagement.
3.4.12 Quality Reporting
The demand for electronic health information exchange among care professionals is growing along with nationwide efforts to improve the quality, safety, and efficiency of health care delivery. Meaningful Use requirements, new payment approaches that stress care coordination, and federal financial incentives are all driving the interest and demand for health information exchange.
CMS implements quality initiatives to assure quality health care for Medicare beneficiaries through accountability and public disclosure. CMS uses quality measures in its various quality initiatives that include quality improvement, pay for reporting, and public reporting.
4 Benefits of HIE
The success of new alternative payment arrangements, including accountable care organizations (ACOs), depends on communicating patient health information well during care transitions. Improved communication is among the most important factors in achieving the quality, satisfaction, and cost goals of these arrangements.22
In a recent literature review, all studies with more rigorous designs found benefits from HIE—fewer duplicated procedures, reduced imaging, lower costs, and improved patient safety. Studies evaluating community HIEs were more likely to find benefits than studies that evaluated enterprise HIEs or vendor-mediated exchanges. Overall, these findings bode well for the HIEs ability to deliver on anticipated improvements in care delivery and reduce healthcare costs.23
4.1 Better Care Coordination
Having a connection to an HIE can help improve the quality of care coordination. An example is a collaborative effort between Quality Insights Mid-Atlantic Renal Coalition (MARC) and Fresenius Medical Center. During this study24, sharing important health information like Blood Stream Infection scores (BSIs) through the HIE helped bridge the information gap between outpatient dialysis providers and hospitals. This information exchange can curtail hospital readmissions, compromised patient safety, or other unintended consequence. This example—using an HIE to obtain results of a blood culture collected in a hospital—shows how an HIE could improve care coordination.
Connecting to an HIE can help improve the quality of care coordination.
4.2 Access to Right Information/Right Time
An HIE’s goal is to deliver electronically the right health information to the right place at the right time. As the ONC website says25 , “Care coordination during unanticipated transitions requires smarter, automated ways for providers to get the health information they need to effectively deliver care. This is where health information exchange comes in: automated alerts and notifications that leverage health information exchange components—such as secure messaging systems and master patient indexes—help providers handle unanticipated transitions by providing them with the right information about the right patient, at the right time.”
Alerting providers through event notifications may improve the quality and efficiency of care among high-risk populations. For example, the Bronx Regional Health Information Organization offers subscription alert services. After an analysis of their services and a survey of their participating organizations with subscription services, preliminary findings26 associated subscriptions alerts with a 2.9% reduced chance that a hospitalized patient would be readmitted within 30 days of discharge. Alert services were associated with saving $2 million in potentially avoided readmission costs in the Bronx for Medicare fee-for-service beneficiaries over a three-year period.
4.3 Fewer Errors and Duplicate Tests and Procedures
Engaging with a HIE can help alleviate many different types of errors and improve quality care. For example, having information on an individual’s medication list through the HIE can help reduce medication errors and eliminate the need for redundant tests or procedures, as described below.
HIEs enable providers to see where a patient has “touched” the health system, reduce duplicate tests and unnecessary paperwork, provide caregivers with clinical notes that allow for more effective care and treatment, review last immunizations, and improve public health reporting. This study27 shows that a provider’s tenure with an HIE can significantly lower the repetitions of therapeutic medical procedures, while diagnostic procedures are not impacted.
Another example28 shows how using the Rochester RHIO HIE system to access previous patient information reduced repeated imaging. HIE system access reduced the adjusted odds of a repeat image by 25%. Of 196,314 patients in the cohort, 34,604 (18%) of patients had at least one imaging procedure, which was equivalent to a rate of 28.7 imaging procedures per 100 patients. Overall, 7.7% of images were repeated within 90 days. If the HIE system was accessed within the 90 days following an initial imaging procedure, imaging was significantly less likely to be repeated (5% repeated with HIE access vs 8% repeated without HIE access, P < .001).
A pilot study found that HIE technology reduced lab tests and radiology exams in three Emergency Departments.
Lastly, a pilot study29 looked to examine the impact of health information exchange technology on reducing laboratory tests and radiology exams in three Western New York Emergency Departments (EDs) supported by HEALTHeLINK. It found much-lower utilization. In the study, all of the patients in a treatment group had access to the HIE platform, while the control group’s care did not include querying an HIE platform.
In one of the ED settings, querying the HEALTHeLINK database was associated with a 52% and 36% reduction in the estimated number of laboratory tests and radiology examinations, respectively. The results indicate that access to additional clinical data through the HIE will significantly reduce the number of laboratory tests and radiology examinations performed in the ED settings—and support the ongoing HIE efforts.
4.4 Improved Population Health
Public health agencies perform health promotion and disease prevention activities using data collected through public health screening and treatment services. They also use data from laboratories, pharmacies, environmental health monitors, emergency medical services, local public health agencies, and clinical care providers. Data collection through a HIE organization can benefit public health functions by increasing the data’s robustness and timeliness. The ONC has several lessons learned30 to consider when engaging a HIE to improve population health.
To best address the health of older adults needing extended or long-term care, LTPAC must fully participate in ACOs and other alternative payment models.
4.5 HIE in LTPAC
LTPAC’s participation in HIE activities has been lagging behind the rest of the healthcare sector for many reasons, including lack of direct incentives. However, ACOs and other alternative payment models, including value-based purchasing, cannot realistically address quality and health outcomes for a growing number of Medicare patients if LTPAC is only marginally involved in these care models, as some early reflections on ACOs have suggested.31, 32
For LTPAC providers to succeed in monitoring and addressing the health concerns of older adults needing extended or long-term care, they must fully participate in ACOs and other alternative payment models.33
Skilled nursing facilities found that HIE improved billing, care planning, and quality of documentation.
When it comes to the benefits of HIE in LTPAC specifically, look to a review by Filipova (2015). Skilled nursing facilities found that the most common benefits of using HIE included faster and more accurate billing to communicate with non-affiliated providers, improved care planning within affiliated organizations, and improved quality of documentation within individual facilities.
HIE also can help reduce costs associated with duplicate testing, as it gives access to a patient’s recent lab work, x-rays, and other test results.34 For example, the systematic review by Rudin and colleagues (2014) found that HIE can sometimes reduce emergency room costs.35
In addition, these HIE features can directly benefit LTPAC providers:
- Subscriptions offered by some HIEs to alert providers of a clinical event. For example, an alert could notify a home care agency to cancel a home care visit when the patient is admitted into a hospital.
- Alerts to track skilled nursing facility (SNF) residents after they are discharged from the SNF, when they show up in an emergency department or a hospital to track 90-day rehospitalization rates and other ACO-based metrics.
- Dashboards and other analytics, including potentially predictive analytics, provided by some HIEs to help with population health and disease progression.
- One-to-one relationship agreements that let HIEs allow LTPAC providers have access to hospital data even before consent is obtained for shared patients.
5 Importance of Governance
Enabling electronic health information exchange requires consensus among multiple stakeholders. Often, complex technical and policy choices are required. Ultimately, governance is established to provide oversight and to hold accountable the parties responsible for exchanging electronic health information.
The Office of National Coordinator for Health Information Technology (ONC) has some guiding principles on HIE governance models and expresses the principles ONC believes are most important for HIE governance. The Governance Framework for Trusted Electronic Health Information Exchange 36(the Governance Framework) is intended to serve as the ONC’s guiding principles on HIE governance. The Governance Framework does not prescribe specific solutions, but it lays out milestones and outcomes that ONC expects as HIE governance entities enable electronic HIE.
5.1 Organizational Principles
The entity that sets HIE policy plays a central role in the success of an electronic HIE initiative. It has a primary responsibility to instill confidence among governed organizations, their users (such as healthcare providers and patients), and other exchange partners in the way electronic exchange is conducted. The ONC believes that an entity that sets HIE policy should do the following37:
- Operate with transparency and openness.
- Establish mechanisms to ensure that the entity adheres to its policies and practices and applicable federal and state laws and regulations.
- Promote inclusive participation and adequate stakeholder representation (especially among patients and patient advocates) in developing policies and practices.
- Ensure its oversight is consistent and equitable.
- Provide due process to the stakeholders it oversees.
5.2 Trust Principles
Trust is a prerequisite for electronic HIE and starts with patients. A lack of trust can jeopardize the initiative’s success. The ONC believes an entity that sets HIE policy is responsible for creating an environment in which patients should do the following:
- Be able to publicly access, in lay person terms, a “Notice of Data Practices.” The notice would explain the purpose(s) for which personally identifiable and de-identified data, consistent with applicable laws, would or could be electronically exchanged (such as treatment, payment, research, quality improvement, public health reporting, population health management).
- Receive a simple explanation of the privacy and security policies and practices that are in place to protect their personally identifiable information when it is electronically exchanged and who is permitted to access and use electronic HIE services.
- Consistent with applicable laws, be provided with meaningful choice as to whether their personally identifiable information can be electronically exchanged.
- Consistent with applicable laws, be able to request data exchange limits based on data type or source (such as substance abuse treatment).
- Consistent with applicable laws, be able to electronically access and request corrections to their personally identifiable information.
- Be assured that their personally identifiable information is consistently and accurately matched when electronically exchanged.
5.3 Business Principles
Successful electronic HIE requires cooperation among all parties. Responsible financial and operational HIE policy is vital to improving care coordination, making healthcare delivery more efficient, and mitigating behaviors that could create proprietary networks and resistance to exchanging information even when it could enhance patient care.
Responsible financial and operational policy is vital to successful HIE.
To ensure that electronic exchange occurs with the patient’s best interests in mind, the ONC believes an entity that sets HIE policy should do the following:
- Set standards of participation that promote collaboration and avoid instances where (even when permitted by law) differences in fees, policies, services, or contracts would prevent patients’ health information from being electronically exchanged.
- Provide open access to exchange services such as directory data that would enable local, regional, and nationwide partners to identify who they can electronically exchange information with and how the exchange could be completed under applicable laws and regulations.
- Publish statistics describing their electronic exchange capacity that include, for example, number of users, the types of standards implemented, number of patient lives covered, and transaction volume.
- Maintain and disseminate up-to-date information about compliance with relevant statutory and regulatory requirements, available standards, potential security vulnerabilities, and best practices developed for HIE.
5.4 Technical Principles
Electronic HIE requires technical conformance at multiple levels. Implementation specifications must be highly specified, rigorously tested, and consistent. An entity that sets HIE policy should promote the following technical conformance and use of standards, according to the ONC:
- Ensure that technology is implemented to support the Trust and Business Principles.
- Prioritize, where available, the exclusive use of federal vocabulary, content, transport, and security standards and associated implementation specifications adopted to support HIE.
- Encourage the use of vocabulary, content, transport, and security standards, and associated implementation specifications developed by voluntary consensus standards organizations (VCSOs) when equivalent federal standards have not been adopted.
- Lead engagement in VCSOs and national efforts to accelerate standards development and consensus on standards adoption and to improve existing standards.
- Work with VCSOs to develop standards for specific use cases and volunteer to pilot and use new standards when no such standards exist.
- Take an active role in developing and implementing conformance assessment and testing methods for HIE and utilize (or promote the use of) testing methods developed to assess compliance with federal standards.
When considering engaging with a HIE entity, it is important to consider these principles. Find out more about ONC’s overall approach to HIE governance and follow continued efforts related to this initiative.
CMS programs encourage eligible professionals and clinicians, hospitals, and critical access hospitals to use certified electronic health record technology.
6 Potential LTPAC Provider Business Models
6.1 CMS Health IT Adoption Incentives Medicare (Medicare and Medicaid)
In 2011, CMS established the Medicare and Medicaid EHR Incentive Programs, now known as the Promoting Interoperability programs. These programs encourage eligible professionals and clinicians (typically physicians and licensed nurse practitioners and physician assistants), eligible hospitals, and critical access hospitals to adopt, implement, upgrade, and demonstrate Meaningful Use of certified electronic health record technology (CEHRT).
Historically, the Promoting Interoperability Programs consisted of three stages:
- Stage 1 set the foundation for the Promoting Interoperability Programs by establishing requirements for the electronic capture of clinical data. These requirements included giving patients electronic copies of health information.
- Stage 2 expanded upon the Stage 1 criteria. It focused on advancing clinical processes and ensuring that the Meaningful Use of EHRs supported the National Quality Strategy’s aims and priorities. Stage 2 criteria encouraged using CEHRT for continuous quality improvement at the point of care and for exchanging information in the most structured format possible.
- Stage 3 was established in 2017 and beyond, after CMS released a final rule in October 2015. The rule focuses on using CEHRT to improve health outcomes. In addition, this rule modified Stage 2 to ease reporting requirements and align with other CMS programs.
For more information about Stage 1 and Stage 2, visit the Requirements for Previous Years on the CMS website.
To continue CMS’s commitment to promoting and prioritizing interoperability of healthcare data, CMS renamed the EHR Incentive Programs to Promoting Interoperability Programs in April 2018. This change moved the programs beyond the existing requirements of Meaningful Use to a new phase of EHR measurement. The programs will have an increased focus on interoperability and improving patient access to health information.
Unfortunately, LTPAC settings are not eligible participants under the incentive program. However, under Medicare, eligible professionals, which include physicians and nurse practitioners, may choose to assign their incentive payments to their employer or to an entity with which they have a contractual arrangement. In exchange, they can access CEHRT.
Under Medicaid, eligible professionals also can assign their incentive payments to their employer or to other state-designated entities. For more information, please see the CMS EHR Incentive Program website and the Frequently Asked Questions on the EHR Incentive Program. For more information about Meaningful Use, applicability to LTPAC settings, and eligibility of LTPAC providers for Meaningful Use incentives, please see this CAST FAQ article.
6.2 State Medicaid Grants
Funding for some state health information exchange activities is already available to states through the Medicaid Electronic Health Records (EHR) Incentive Program. The American Recovery and Reinvestment Act of 2009 authorized the program at the 90% match rate through 2021. Within the parameters set by State Medicaid Director (SMD) Letter #11-004 and SMD Letter #10-016, states may request 90/10 Health Information Technology (HITECH) administrative funding for a wide range of HIE activities that support providers’ adoption and Meaningful Use of EHRs.
States may request 90/10 Health Information Technology (HITECH) administrative funding for a wide range of HIE activities.
While the above approach is specific to existing Medicaid authorities, states are highly encouraged to engage with CMS on other opportunities to further build infrastructure and policies that drive health information exchange utilization.
States can leverage opportunities like State Innovation Model grants and Demonstration Grant for Testing Experience and Functional Assessment Tools to further expand health information exchange capabilities where current policies are limited. CMS will continue to work with states as these opportunities become available.
6.3 Potential Affordable Care Act (ACA) Opportunities
The Affordable Care Act (ACA) is shifting the healthcare system in the U.S. away from the traditional fee-for-services to a pay-for-performance system. Moreover, CMS is moving to reimburse Medicare Certified Home Health on a value-based purchasing model instead of a prospective payment model. This shift is starting to eliminate the misalignment of incentives in traditional Medicare, Medicaid, and private insurance programs.
The ACA puts explicit emphasis on the use of health information technology.
There are many provisions and models in the ACA that would benefit from care planning and coordination technologies and services, as well as encourage their adoption. The act created the Center for Medicare & Medicaid Innovation (CMMI), which explores new care delivery and payment models and initiatives that do the following:
- Use more holistic, patient-centered, and team-based approaches to chronic disease management and transitional care.
- Improve communication and care coordination among care providers.
- Improve care quality and population health while reducing growth in expenditures.
The act puts explicit emphasis on the use of health information technology (health IT). It focuses on care planning and coordination technologies, health IT in health homes for enrollees with chronic conditions, the Independence at Home Demonstration, and the use of technology in new state options for long-term services and supports. These initiatives include the following:
- Hospital Readmission Reduction Program (HRRP).
- ACOs.
- Bundling of Payments models, of which Retrospective Acute Hospital Stay and Post-Acute Service are relevant to LTPAC providers.
LTPAC providers bring a significant value for hospitals, physician groups, payers, and ACO partners by providing the following services:
- Rehabilitation and skilled nursing facilities provide post-discharge/post-acute patient rehabilitation.
- Skilled nursing facilities, assisted living facilities, continuing care retirement communities, housing with services, and home health agencies provide post-acute patient stabilization and sub-acute chronic disease management.
- LTPAC provides holistic person-centered care, including support services.
- LTPAC offers lower-cost care settings than hospitals.
These new care delivery and payment models will enable LTPAC providers who use technologies, like care planning and coordination technologies, to derive revenue sources from strategic partners. The following white paper, The importance of home and community-based settings in population health management, offers some key questions LTPAC providers should discuss with their acute care partners.
6.4 Private Pay
Other payment sources for engaging with a health information exchange entity may include private pay by the provider.
6.5 Standard of Care and Other Payment Sources
LTPAC and community health providers, special population agencies, self-pay and self-insured organizations, and others, especially not-for-profits, may engage with a health information exchange entity to enhance their standard of care. Grants may cover these services. Or the organization may absorb the cost, with different revenue sources covering it, including charitable contributions.
6.6 Return on Investment (ROI) of HIE
Among health information exchange’s benefits are potential financial savings to different stakeholders, including patients and/or their families, payers, care providers, etc.
However, the financial savings and return on investment (ROI) depend on a number of factors. These include the care delivery model, the payment/reimbursement model, the technology used, and of course costs. The first and most important step in calculating ROI is to consider the different stakeholders, identify the investors, and calculate the gains and savings netted/accrued to each investing stakeholder under each particular care delivery and payment model.
The financial savings and ROI depend on a number of factors.
When calculating ROI, one should only include the gains that accrued to that particular stakeholder minus all expenses, relative to that stakeholder’s own investment/cost. Often the reduction of hospital days is erroneously included in the providers’ ROI, which is not true under the traditional fee-for-service reimbursement model and can be misleading. Such a reduction usually accrues to the payer.
6.7 ROI to Patients and/or Their Families
ROI to patients and/or their families can be calculated as follows:
![]()
For private pay patients and their families, for example, the financial gains of HIE-facilitated care coordination lie in prolonging independence by maintaining health. Good health may prevent disability and avoid the need to move into assisted living or skilled nursing facilities. These benefits are significant.
The gains may also include savings in co-pays for recurring hospital visits, and of course a higher quality of life, which is difficult to quantify. The patient’s and family’s expenses are the monthly out-of-pocket of private care services, plus any co-pay for the occasional physician office visit, lab tests, and prescriptions.
6.8 ROI to Payers
ROI to payers can be calculated as follows:
![]()
For dual Medicare and Medicaid eligible patients who are nursing home eligible, for example, the financial gains of HIE-facilitated care coordination under a Medicaid Managed Care program that accrue to program depend on keeping patients in their own homes with home health, home care, and other supportive services. Otherwise, the managed care would be liable for the costs of nursing home room and board.
Managed care’s investment is the monthly rate of care coordination, as well as home- and community-based supportive services aimed at keeping the patient independent. Additional savings, like reductions in hospitalization and hospital readmission costs, may accrue to Medicare or the managed care plan. These savings or gains should be correctly attributed.
6.9 ROI to Care Provider
ROI to care providers can be calculated as follows:
![]()
The care provider who makes investments in information and communications technology infrastructure, care planning and coordination technology, and HIE subscription fees and who offers care coordination and management services may reap the following benefits:
- Lower costs in delivering the same services, including staff efficiencies and staff travel costs (if the payer covers the remote services, rather than just the in-person visit).
- Higher reimbursements/payment from the payer or strategic partner as incentive payments for avoiding more costly care settings, procedures, events, or penalties.
For example, an LTPAC provider partnering with a physician group ACO to manage a chronically ill patient population can potentially get a percentage of the incentives or shared savings payments the ACO receives from the payer for reducing hospitalizations and hospital readmissions as a result of participating in HIE, which can be significant for certain populations.
- The LTPAC provider’s net gain is the sum of all gains accruing to the LTPAC provider in staff efficiencies, increased referrals from the ACO, traditional fee-for-service payments for eligible services, and additional incentive payments received from the ACO, minus the costs of care coordination technology, HIE subscription fees, and actual costs of services delivered.
- The physician group ACO’s ROI is the portion of the payer’s incentive payment that they get to keep, plus any additional fee-for-service payments due to more frequent office-based services, minus the actual costs of services they deliver (for example, in medication reconciliation), relative to the portion of incentives they pass through to the LTPAC provider.
A contrast is a partnership between an LTPAC provider and hospital under the traditional fee-for-service model. For example, the LTPAC provider may help its hospital partners reduce 30-day readmission rates for pneumonia, congestive heart failure, and heart attack patients, helping the hospital avoid Medicare’s payment penalties under the Hospital Readmissions Reduction Program.
The hospital may contract with and pay the LTPAC provider a percentage of the penalties saved for delivering better coordinated care that reduces 30-day readmissions for patients discharged from the hospital after being admitted for pneumonia, congestive heart failure, or heart attack.
- The LTPAC’s net gain is again the sum of all gains accruing to the LTPAC provider in staff efficiencies, increased referrals from the hospital, traditional fee-for-service payments, and additional payments received from the hospital, minus the costs of care coordination technology, HIE subscription fees, and actual costs of services delivered.
- The hospital’s ROI is the portion of avoided penalties it gets to keep, plus any additional fee-for-service payments it gains for more referrals due to improved quality ratings, minus the actual costs of services the hospital delivers, relative to the portion of avoided penalties it passed through to the LTPAC provider, plus any additional costs incurred for staff time in care coordination, medication reconciliation, or health information exchange.
6.10 Online ROI Calculator
Once individual investors have been clearly identified, an estimate of the ROI to the different stakeholders can be calculated. The SCAN Foundation has recently published a white paper on making the business case for person-centered care with instructions for using an ROI calculator they developed.
This ROI calculator is designed to quantitatively assess the business case for person-centered care (PCC) programs that serve older adults with chronic conditions and functional limitations. PCC programs are ones where individuals’ values and preferences are elicited and, once expressed, guide all aspects of their healthcare, supporting their realistic health and life goals.
This ROI calculator quantitatively assesses the business case for person-centered care programs that serve older adults with chronic conditions and functional limitations.
This type of care is achieved through a collaborative relationship and decision-making process among the person, their chosen supports, and their medical and social service providers. As discussed in detail above, the business case for PCC involves weighing the costs of offering this approach to care against the benefits expressed in dollar terms. Benefits accrue principally in the form of avoided medical utilization, but also potentially in the form of higher revenues.
With the ROI calculator, the user can create optimistic and pessimistic scenarios and compare the results.
The ROI calculator has a number of practical features:
- Risk Stratification: The population that is suitable to receive PCC can be segmented into high and moderate risk categories. The ROI will be likely a higher percentage for the segment that is at higher risk for medical utilization. The calculator can show how limited the offering must be if a specific return were being sought.
- Potential Revenue from PCC: The calculator allows for PCC program offerings to incorporate possible revenue enhancements in addition to the more probable benefits resulting from reducing costs.
- Slider Bars: This feature allows the user to compute instantaneous “what-if” calculations by changing values of inputs and immediately viewing these new inputs’ influence on the ROI.
- Flexibility in Expressing Variables: All variables can be entered by the user in terms of their convenience—per person, per month, or per year. Hospital admissions, for example, are generally reported on an annual basis, and encounters with a social worker or nurse practitioner are often expressed on a monthly basis. The calculator automatically converts rates and volumes, no matter how expressed, into a common per member per month measure.
- Scenarios: This feature allows ROI comparisons across different programs as well as varied constellations of input values. For example, the user can create optimistic and pessimistic scenarios and compare the results. Sometimes even the pessimistic scenario can yield an acceptable result for the ROI.
- Accounting for Uncertainty: Admittedly, some key determinants of the ROI are not known with certainty. Therefore, a “Monte Carlo” simulation that accounts for uncertainty with respect to the magnitudes of key variables is an optional part of the tool. This simulation recognizes this uncertainty and displays accordingly a reasonable range of results for the ROI rather than a single deterministic value. The tool also quantifies the strengths of the separate influences each variable has on the resulting ROI.
- Other Metric – Payback Period: In addition to the ROI result, the calculator displays the payback period–the number of months the PCC program would need to operate (assuming a positive operating margin) for any initial investment to be recouped. This metric may be useful for programs involving substantial up-front launch costs.
- Threshold Analysis: A user can conduct a threshold analysis and query the calculator on questions such as the following: What is the maximum amount that can be spent on PCC so that the program does not lose money? Or for a given cost of delivering PCC, how effective must it be in reducing certain events, such as hospital readmissions, to generate a required (hurdle) level of ROI?
To access the calculator tool, go to The SCAN Foundation.
7 Planning for and Selecting Appropriate HIE
Planning to engage in HIE is a strategic decision that should be part of an organization’s strategic planning and strategic IT planning efforts.
A multidisciplinary team that includes management, clinicians, IT, and departments that would contribute or use any of the exchanged data should do the planning. Sometimes teams would include the technology vendors—for example, EHR, care planning and coordination software, and telehealth vendors—and any third-party system integrators or facilitators the organization may need. Representatives of partner organizations with whom the organization will exchange information should also be included.
7.1 Visioning and Strategic Planning
Start the journey with the organization’s strategic plan as a guide. Some of your organization’s strategic goals would dictate a number of things that can help you plan for your HIE participation. These may include the following:
- Specific programs to serve certain populations, where they live, and who provides them with healthcare and support services.
- Strategic partners key to success, and their area of service.
- Partners’ adopted health IT technologies (EHR, referral management, or care planning and coordination platforms), their interoperability and HIE participation and capabilities.
- The specific data they need from your organization, and the data you need from them. Your adopted health IT technologies (EHR, referral management, or care planning and coordination platforms), and their interoperability and HIE capabilities.
You may need to work with middleware developers and integration engine/system integration third parties, and you may need to participate in more than one HIE.
It is best to do this during strategic planning and for all your strategic goals. Remember, given the current state of interoperability, you may need to work with middleware developers and integration engine/system integration third parties, and you may need to participate in more than one HIE. This scenario is definitely true for multi-state multi-site organizations, but it is sometimes true for single sites with different programs, partners, and HIE needs.
7.2 Organizational Readiness Assessment
Planning for and implementing a health information exchange program is a complex and time-consuming endeavor. It requires a robust team, time, resources, and dedication.
7.2.1 IT Infrastructure
A comprehensive inventory of IT infrastructure components is critical to developing a technology plan. Knowing the current state of technology today will ensure that its configuration and scalability will sustain the organization into the future. Ensure your IT infrastructure has redundancies built in, both in architecture and in having dual internet service providers to ensure that your organization can connect to the HIE.
7.2.2 Available EHR Solution
When considering engaging with a HIE entity, it’s important to work along with your current EHR and other health IT vendors to ensure a connection can be made to that HIE. There may be different versions of an EHR platform that are supported and others that are not. Be specific, and don’t shy away from reaching out to your vendor.
7.2.3 Available Data
Review the available data elements that your organization is willing to potentially share. Consider the information you would like to capture by engaging with a HIE entity. Make sure it is semantically interoperable and has the same meaning as the HIE’s system .
In most cases, the data shared is a function of the EHR product. A Consolidated Clinical Document Architecture (C-CDA) is normally configured by the product, in terms of the included data fields. Changes to the default settings are usually difficult. EHRs that ONC have accredited as “certified” are required to have certain interoperability functionality. For example, PointClickCare is certified and is fully capable of exchanging C-CDAs.
Consider how you can take advantage of new data elements to improve your care quality and outcomes and redesign your workflows.
7.2.4 Additional Data Needed and Sources
Think about the data or notifications your organization would like to start receiving as you connect to an HIE. You can exchange many different types of data with a HIE, and many types are real-time. Exchanging this data can have significant implications for your organization and can change your workflows drastically. An example is admission notification of a patient or client you have just discharged. Consider how you can take advantage of these new data elements not only to improve your care quality and outcomes, but also to redesign your workflows to maximize efficiencies and bottom line.
7.2.5 Interoperability/ Interfacing Capability
Interoperability means that two disparate systems are able to communicate with one another to exchange data. To end users and many in the industry, interoperability means every product works with others seamlessly. Unfortunately, not even the most highly integrated suite of components in a product fully does so.
When modules or components are integrated, they generally have been built by the same group that did the original development and programming, have similar design characteristics, and can exchange most data. In general, the components or modules in highly integrated suites of products work well together, but they will not work with any other vendor’s product without specialized interfacing .
Recently we have seen unprecedented efforts to develop, implement, and use interoperability standards and standard data elements in EHRs to support interoperability. Many EHR vendors have created APIs to get data out of systems and support interoperability, interfacing, and information exchange between systems and providers.
In addition, today we see many third-party system integrators and middle-ware developers that have built bridges between systems to support information exchange. Many HIE entities work with such third-party vendors as well. Make sure your HIE works with your EHR vendor, and your partners’ EHR vendor(s), either directly or through a third-party intermediary.
7.2.6 Consent Management
HIEs help route information among various participating providers. In some HIEs, a provider can send out a broadcast query that asks all provider participants whether they have information on a particular patient. This method of asking for patient information is different from one provider directly contacting another to request a patient’s information.
As electronic HIE increases, patient trust in HIEs must be ensured.
As electronic health information exchange increases, patient trust in HIEs must be ensured. Patients may more frequently be asked to make a “consent decision” that concerns the sharing and accessing of the patient’s health information through an HIE for treatment, payment, and healthcare operations purposes. Consent decisions may allow patients to determine the following, depending on the electronic HIE taking place:
- If their health information will be released,
- Under what circumstances the release will take place (any time or emergencies only?), and
- By whom (Healthcare providers? HIEs?).
Providers may choose to offer one or a combination of the following general types of consent policies:
- Opt-in: Default is that patient health information is not shared. Patients must actively express their consent to share.
- Opt-out: Default is for patient health information to be automatically available for sharing. Patients must actively express their desire to not have information shared if they wish to prevent sharing.
Patients may choose to give providers and HIEs full access to their information, limited access, or no access at all. When patients are asked to make consent decisions, providers, HIEs, and other health IT implementers should help patients make the consent decision meaningful.
LeadingAge CAST has Cybersecurity Resources to address cybersecurity concerns.
7.2.7 Cybersecurity
Cybersecurity is an important area to consider when engaging with health information exchange. LeadingAge CAST has Cybersecurity Resources available to address these concerns. The Cybersecurity Resources were created to help LeadingAge members and other aging services organizations understand cybersecurity threats, how to mitigate these threats, and how to respond if attacked. The resources include a Cybersecurity White Paper, case studies, and a benchmarking questionnaire that will help providers identify where they may be at risk, so that they can work to plug those vulnerabilities.
7.2.8 Policies and Procedures
Selecting and implementing various types of HIE technologies will affect existing policies and procedures, which will have to evolve to support whatever type of technology the organization selects. Consultants and vendors who specialize in helping long-term care facilities with business process reengineering can address these challenges and opportunities.
7.2.9 Partner Assessment
Selecting a technology partner dedicated to innovation is the first step. There are a lot of technology “vendors.” Choose a partner instead. Good partnership requires deep resources to create a positive experience for all aspects of an organization. Selecting a partner who is dedicated to innovation and a convergence strategy, who can assist in evaluating workflow and processes, and can deliver both mobility and resident engagement technologies, is important to the partnership’s overall success.
According to a technology provider addressing the future of senior living, “While investing in new and advanced forms of technology for senior living facilities can be expensive and time consuming, it is critical to staying relevant in the industry and meeting the growing demand of residents. As communities look at new projects or go through re-financing on existing communities, it is important to engage technology experts and include forward-thinking solutions in the budget planning process.”
It is important to learn about the types of HIE entities available.
7.2.10 Available Technology Solutions
It is important to learn about the types of HIE entities available, how they function, their uses and benefits, their high-level network requirements, and the connectivity they require. With the ideal systems in mind, consider the type(s) of solutions needed and questions that include the following:
- Does the HIE service your location?
- Does the HIE support notifications and alerts, such as Emergency Room admissions?
- What types of data do you want to exchange?
- What kinds of services are you interested in?
- Does the technology integrate, interface, or interoperate with existing technologies, such as your EHR?
7.2.11 Operating Environment
The operating environment includes the care setting, the state in which the community is located, and the applicable federal and state regulations.
7.3 Operational and Programming Planning
7.3.1 Project Team
Operations team members will play a key role in implementation success, as they are the most connected to the people they serve. Ensure that operational leadership has buy-in early, and work alongside these leaders to identify the best people in the field to become evangelists. The key to engaging field operations—such as nurses, billing, certified nursing assistants, and administrative staff— in the initiative’s goals is that they are not salespeople; they are the connection evangelists.
7.3.2 Goal Setting
Defining the HIE goals is critical to measuring success. Each organization will have different ideas of what success looks like based on strategic goals and internal operations. Before starting an HIE technology program, the organization should set a clear series of goals and metrics. Goals should be measurable and routinely reported on within the organization’s operations. Ensure that they are SMART goals:
- Specific.
- Measurable.
- Attainable.
- Realistic.
- Trackable.
Setting both short-term and long-term goals for the HIE technology program is highly recommended. Organizational goals set at the program’s start will likely be different six to 12 months post implementation. The goals should be evaluated continuously and updated as programs change. It is also important to understand that a new program will have the ability to achieve several major goals during its initial adoption.
Set both short-term and long-term goals for the HIE technology program.
7.3.3 Program Design
HIE programs should be designed with the organization’s short- and long-term goals in mind to help ensure success. Each program’s design should always consider how to align objectives, strategies, and technical plans by using HIE technology. Be sure to share experiences from other similar organizations to assist in strategies to build a HIE program within the organization or strengthen an existing one. Before starting any program, clearly define the new model of care and prepare staff with training and support plans.
7.3.4 Technology Review and Selection
Once an organization has completed the visioning and strategic planning exercise, assessed organizational readiness, assembled the project team, set the project’s goals, and designed the program, the team needs to develop a set of detailed technology requirements. These criteria will be used to review and select the appropriate HIE solution.
Location, Modality of Exchange, and Type of HIE
The planning process would help identify key requirements that should include the following:
- The location (state) where the organization wants to deploy the HIE solution.
- The modality of exchange, whether it is Direct Push Exchange, Query-Based (Pull), or Consumer Mediated Exchange.
The type of HIE entity and network is also a consideration, which may include the following:
- National HIE Networks
- State HIEs
- Regional HIEs
- Private/Proprietary HIEs
- • Hybrid Networks
Type of Data Exchanged
Type of data exchanged should also be considered and may include one or more of the following:
• Admission, Discharge, Transfer (ADT)
• Demographics
• Care Plan
• Allergies
• Medication List
• Problem List
• Status, Background, Assessment, and Recommendations (SBAR)
• Electronic Interventions to Reduce Acute Care Transfers (INTERACT)
• Admission Form
• Discharge Summary
• Functional Assessment
• Cognitive Assessment
• Physician Orders for Life-Sustaining Treatment (POLST)
• Patient’s Advance Directives
• Electronic Reporting of Immunizations
• Laboratory Results
• Imaging Exchange
• Public Health Reporting
• Consolidated Summary EHR from Other Providers
Services Offered
The value-added service offered is also a consideration and may include one or more of the following:
• Consolidated Clinical Summary Record Exchange
• Patient Centered Data Home (Regional and National Networks Only)
• Health Information Services Provider (HISP)
• Electronic Authentication as Shared Service
• Patient Matching (Master Patient Index)
• Provider Directory
• Consent Management
• Quality Reporting
• Proactive Alerts/Push Notifications
• Referral Services
• Patient Access/Portal
• Export to Personal Health Record (PHR)
Communication Method, LTPAC EHR Supported, and Consent Policies
The type of communication method is also a consideration and can include one or more of the following:
• Secured Web Services (Example: Fast Health Information Resources (FHIR))
• TCP/IP over VPN
• Secured File Transfer Protocol (FTP)
• Secure E-Mail (Example: Project DIRECT)
The LPTAC EHR supported is also a consideration. Ideally, the HIE entity you choose supports your current EHR. If it does not, you should explore if the HIE works with a third party that can help you interface to the HIE, or if your EHR vendor can work directly with the HIE or any of their third-party partners.
The consent policies are also a consideration, whether the system has an opt-in or opt-out policy.
7.3.5 Implementation
The implementation and planning phase takes the information gained by the assessment phase and begins to answer the “who,” “how,” and “when” questions. During this phase, you identify the executive steering committee members and create a project charter. Set aside enough time for this phase, as it is involved and detailed.
Contingency planning is part of the overall plan; the team must assess and identify potential risks throughout the project and deal with them quickly. Most often, risk is not going to severely impact the project. However, when a risk that could impact the project’s timeline, budget, or goals appears, the steering committee should be made aware to make decisions.
It is important to provide continuous monitoring of any program.
7.3.6 Post-Implementation Monitoring
It is important to provide continuous monitoring of any program. Monitoring validates the program, tracks improvement, and identifies any new problems that may occur. Measuring the program’s quality will provide an opportunity to establish its positive impact on the organization, consumers, and any partners. If post-monitoring does not show significant differences in care planning and coordination for the people served, the organization will need to rethink the program.
8 Role of System Integrators
The fundamental concern in health information exchange is integrating health information across distributed, heterogeneous, and disparate information systems. Healthcare organizations have
attempted various approaches to solve the problems associated with integration. An evaluation of information systems examines the various approaches to system integrators and categorizes these technical approaches:38
- Message-Oriented Integration
- Application-Oriented Integration
- Coordinated-Oriented Integration
- Middleware-Oriented Integration
8.1 Message-Oriented Integration
Message-oriented integration relies on a set of standard messages that allow various health information subsystems to exchange messages carrying data. This approach uses databases, APIs, and data exchange to produce information. The primary idea is to exchange structured electronic messages between different applications and use already-established standards.
Message-oriented integration supplies functional integration of health information at a regional level.
It is considered a mechanism that supplies functional integration of health information at a regional level in order to automate medical processes such as patient admission, transfer, prescriptions, and ordering of laboratory and radiological examinations, for automatic or on-demand receipt of results. This approach provides an effective way to solve the basic integration problems between information systems; however, it does not cover true interoperability and integration of information.
The health information still looks like “islands” of systems with a lack of interoperability and communication. The problem is with increasing the number of possible interactions between systems, the limitations of scalability become apparent. Also, despite using medical standards, the implementation still varies and is vendor dependent.
This solution cannot be considered as system integration but rather as inter-system communication. In healthcare, message-oriented integration approaches are seen in the use of HL7, DICOM messages, EAI, XML DTD8, and HL7 CDA documents.
8.2 Application-Oriented Integration
Application-oriented integration supplies a layer of defined and centrally managed applications on top of existing applications in order to support the flow and exchange of information and control logic between them by combining relevant applications and processes. This solution often consists of process engines, workflow or distributed objects, and integration servers. It is essential to define and understand the application and processes in the organization to provide application-oriented solutions.
Workflow-oriented Integrating the Healthcare Enterprise (IHE) integration profiles are an example of an application-oriented integration approach. IHE defines the Technical Framework to achieve system integration by describing implementation of already existing medical standards, integration profiles, and detailed technical specification of actors and transactions.
Actors, in this technical framework, are information systems or component parts of information systems that provide, act, produce, manage, or operate on categories of information needed by operational activities in the enterprise.
Transactions describe interactions between actors that transfer the needed information via standards-oriented messages. Integration profiles are identified as a set of IHE Actors which involved in a medical information process and interact through transactions to perform specific operations.
The main goal is to ensure all information needed in decision making is available on time and is accurate for the users of medical software application and medical tasks.
8.3 Coordinated-Oriented Integration
Coordinated-oriented integration provides a consistent view on the information held in several separate and disparate systems, applications, and underlying services for the user. This can be supplied by using a unified front-end system or by synchronizing and coordinating the various systems or applications on the user workstation.
Coordinated-oriented integration provides a consistent view on the information held in several separate and disparate systems, applications, and underlying services.
When a user signs onto one system within the tied group of disparate systems by this approach, the same sign-on is simultaneously executed on all other systems within the group. This solution builds a combined view of the information at the desktop and/or portal level in a unified way. This approach emphasizes end-user aspects. The systems or applications are not necessarily directly integrated on a service or data level. Examples of this approach include the CCOW9 context management standard from HL7, healthcare professional portals, and IHE Patient Synchronized Applications (PSA)
This division of integration approaches addresses the classification of specific integration needs (relating identified interoperability requirements to different integration approaches) and identification of relevant standards and specifications. In many cases, the solution is the combination of features from different integration approaches, but it is useful to define the primary approach as one of the specified options.
8.4 Middleware-Oriented Integration
Middleware-oriented integration defines a set of services, interfaces, or shared methods that support the entire system. This approach provides the infrastructure for sharing functional services and information. Services are well defined and self-contained functions that do not rely on the context or state of other services.
Services may be implemented using a wide range of technologies, including SOAP, DCOM, CORBA, Java or Web Services. This approach reduces the need for replication of data and methods in several systems and enables them to operate by providing infrastructure for Message and Application oriented integration.
The generic middleware components can provide interconnection and integration of health information. Healthcare organizations can be assumed to be a collection of disparate users that are performing diverse tasks. All require the sharing of a common data set and use of a common business services set. These must be accessible to applications by standard interfaces. The middleware-oriented integration approach addresses this subject. This solution may require changes in legacy systems such as adaptation into the common infrastructure.
For more information, please see this study.
9 HIE Matrix Components
The HIE Selection Matrix has 11 sections to help organizations narrow the possible products:
- Service Location
- Modality of Exchange
- Type HIE Entity
- Type of Data Exchanged
- Services Offered
- Communication Method
- LTPAC EHR Supported
- Consent Policies
- Company Experience
- Contact Information
- Strengths
The HIE Selection Matrix includes the following sections:
Service Location
Service Location illustrates states in which services are provided. All 50 states are listed.
Modality of Exchange
Modality of Exchange illustrates the three different types of exchange:
- Direct Push Exchange (Direct Sharing)
- Query-Based/Pull Exchange (Indirect Sharing)
- Consumer Mediated Exchange
Type of HIE Entity and Network
This category includes the following options:
- National HIE Network
- State HIE
- Regional HIE
- Private/Proprietary HIE
- Hybrid Network
Type of Data Exchanged
This category includes options for the following options for types of data exchanged:
- Admission, Discharge, Transfer (ADT)
- Demographics
- Care Plan
- Allergies
- Medication List
- Problem List
- Status, Background, Assessment, and Recommendations (SBAR)
- Electronic Interventions to Reduce Acute Care Transfers (INTERACT) Admission Form
- Discharge Summary
- Functional Assessment
- Cognitive Assessment
- Physician Orders for Life-Sustaining Treatment (POLST)
- Patient’s Advance Directives
- Electronic Reporting of Immunizations
- Laboratory Results
- Imaging Exchange
- Public Health Reporting
- Consolidated Summary EHR from other providers
Services Offered
This category includes the following options:
- Consolidated Clinical Summary Record Exchange
- Patient Centered Data Home (Regional and National Networks Only)
- Health Information Services Provider (HISP)
- Electronic Authentication as Shared Service
- Patient Matching (Master Patient Index)
- Provider Directory
- Consent Management
- Quality Reporting
- Proactive Alerts/Push Notifications
- Referral Services
- Patient Access/Portal
- Export to Personal Health Record (PHR)
- Other; please list
Communication Method
This category includes the following communication methods:
- Secured Web Services (Example: Fast Health Information Resources (FHIR))
- TCP/IP over VPN
- Secured File Transfer Protocol (FTP)
- Secure E-Mail (Example: Project DIRECT)
LTPAC EHR Supported
This category includes which LTPAC EHR are supported:
- ADS Data Systems
- Afoundria
- American Data
- American HealthTech
- BlueStrata EHR
- Cantata Health
- Cerner Extended Care
- Eldermark
- GEHRIMED
- HCS
- LG CNS
- LINTECH
- MatrixCare
- MED e-care
- Healthcare Solutions, Inc.
- Momentum HealthWare
- Netsmart
- New Tech Computer Systems
- PointClickCare
- SOS Corporation
- VorroHealth
- Yardi
- Other; Please List
Consent Policies
This category includes the following consent policies options:
- Opt-In
- Opt-Out
- Notes
Company’s Experience and Viability
This area includes the following:
- Number of Years in Business
- Number of Users (Regardless of Setting)
- Core Customer Base, Focus of Line of Business
- Link/s to Additional Case Study/ies
Contact Info
This section includes the following items:
- Main Membership Contact Name
- Phone Number
- E-mail Address
- Membership Inquiries URL
- LTPAC Membership Fee
Strengths
The last section of the matrix is dedicated to the following:
- Strengths
- Areas for Improvement
- Ongoing Development
- References
10 Acknowledgement of Contributors
10.1 Workgroup Members
- Alexandra Fitz Blais, NYeC
- Carianne Borut, NYeC
- Majd Alwan, LeadingAge CAST
- Nicole Casey, NYeC
- Ryan Bramble, CRISP
- Scott Code, LeadingAge CAST
10.2 Writing Workgroup Members
- Alexandra Fitz Blais, NYeC
- Carianne Borut, NYeC
- David Finkelstein, Hebrew Home at Riverdale
- Jill Eisenstein, Rochester RHIO
- Kelly Thompson, SHIEC
- Majd Alwan, LeadingAge CAST
- Nicole Casey, NYeC
- Ryan Bramble, CRISP
- Scott Code, LeadingAge CAST
- Sharon L. Muscatell, SHIEC
- Steve Rottmann, WISHIN
11 References and Resources
1. SHIEC. (2019). HIE 101 – SHIEC. [online] Available at: https://strategichie.com/resources/hie-101/#1519863086641-adb25ac0-eb35 (No Longer Available)
2. Healthit.gov. (2019). What are the different types of health information exchange? | HealthIT.gov. [online] Available at: https://www.healthit.gov/faq/what-are-different-types-health-information-exchange
3. Office of the National Coordinator (2012). HIE DRIVEN SUBSCRIPTION AND NOTIFICATION SERVICES: MARKET ASSESSMENT AND POLICY CONSIDERATIONS, p.3. https://archive.healthit.gov/sites/default/files/hie_subscription_notification_final.pdf
4. Ibid, p.7
5. Office of the National Coordinator (2012). QUERY-BASED EXCHANGE: KEY FACTORS
INFLUENCING SUCCESS AND FAILURE, pp. 8-9. https://archive.healthit.gov/sites/default/files/query_based_exchange_final.pdf
6. Healthit.gov. (2019). What are the different types of health information exchange? | HealthIT.gov. [online] Available at: https://www.healthit.gov/faq/what-are-different-types-health-information-exchange
7. https://www.healthit.gov/topic/health-it-initiatives/blue-button
8. Miliard, M. (2018). How Apple’s Health Records could reshape patient engagement. [online] Healthcare IT News. Available at: https://www.healthcareitnews.com/news/how-apples-health-records-could-reshape-patient-engagement
9. https://carequality.org/what-we-do/
10. https://ehealthexchange.org/
11. https://ehealthexchange.org/onboarding/hub/
12. https://strategichie.com/initiatives/pcdh/
13. https://www.cms.gov/newsroom/press-releases/cms-accountable-health-communities-model-selects-32-participants-serve-local-hubs-linking-clinical
14. https://www.epic.com/interoperability/ehr-interoperability-from-anywhere
15. https://www.commonwellalliance.org/about/
16. Monica, Kate. (2017) Providers Caring for an Aging Population need Widespread HIE Use. [online] EHR Intelligence. Available at https://ehrintelligence.com/news/providers-caring-for-an-aging-population-need-widespread-hie-use)
17. Ibid
18. Johnson C., Pylypchuk Y. & Patel V. (December 2018). Methods Used to Enable Interoperability among U.S. Non-Federal Acute Care Hospitals in 2017, no.43. Office of the National Coordinator for Health Information Technology: Washington DC.
19. https://www.healthit.gov/sites/default/files/page/2019-02/HITACNPRMPresentation.pdf
20. https://www.ehidc.org/sites/default/files/resources/files/2019%20HIE%20Survey_eHealth%20Initiative_final.pdf
21. https://www.healthit.gov/sites/default/files/onc-beacon-lg1-adt-alerts-for-toc-and-care-coord.pdf
22. Berwick, D. M., T. W. Nolan, and J. Whittington. The Triple Aim: Care, Health, and Cost. Health Affairs 27, no. 3 (2008): 759–69.
23. Menachemi N, Rahurkar S, Harle CA, Vest JR. J Am Med Inform Assoc. 2018 Sep 1;25(9):1259-1265. doi: 10.1093/jamia/ocy035. The benefits of health information exchange: an updated systematic review. Available at: https://www.ncbi.nlm.nih.gov/pubmed/29718258
24. Closing the information gap: Health information exchange in dialysis. Healio Nephrology News & Issues. Available at:
https://www.healio.com/nephrology/practice-management/news/online/%7B0f6f8016-a39b-4e1b-b7eb-dac1b8f678ca%7D/closing-the-information-gap-health-information-exchange-in-dialysis
25. Galvez, Erica. (March 22, 2013) HIE Bright Spots: Health Information Exchange as a Key Enabler of Care Coordination – Part 1. [online] Health IT Buzz. Available at: https://www.healthit.gov/buzz-blog/state-hie/hie-bright-spots-health-information-exchange-key-enabler-care-coordination-part-1
26. Hospitalization event notifications and reductions in readmissions of Medicare fee-for-service beneficiaries in the Bronx, New York. Mark Aaron Unruh, Hye-Young Jung, Rainu Kaushal, Joshua R Vest Journal of the American Medical Informatics Association, Volume 24, Issue e1, April 2017, Pages e150–e156, https://doi.org/10.1093/jamia/ocw139 Published: 07 October 2016
27. Do Health Information Exchanges Deter Repetition of Medical Services? Saeede Eftekhari, Niam Yaraghi, Ranjit Singh, Ram D. Gopal, Ram Ramesh. University of Connecticut School of Business Research Paper No. 17-03 https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2971503
28. Am J Manag Care. 2014 Nov;20(11 Spec No. 17):eSP16-24. Health information exchange and the frequency of repeat medical imaging. Vest JR1, Kaushal R, Silver MD, Hentel K, Kern LM. https://www.ncbi.nlm.nih.gov/pubmed/25811815
29. Yaraghi N. J Am Med Inform Assoc. 2015 Nov;(6):1169-1172. doi: 10.1093/jamia/ocv068. An empirical analysis of the financial benefits of health information exchange in emergency departments. Available at: https://academic.oup.com/jamia/article/22/6/1169/2357674
30. Healthit.gov (September 2017). Connecting Public Health Information Systems and Health Information Exchange Organizations: Lessons from the Field | HealthIT.gov. [online] Available at: https://www.healthit.gov/sites/default/files/FINAL_ONC_PH_HIE_090122017.pdf
31. Crecelius, C. “Accountable Care Organizations and the Long Term Care Physician.” Caring for the Ages 14, no. 7 (2013): 16–17.
32. Byrne, C., Dougherty, M. Long-Term and Post-Acute Care Providers Engaged in Health Information Exchange: Final Report. Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, Office of Disability, Aging, and Long-Term Care Policy, 2013. Available at http://aspe.hhs.gov/daltcp/reports/2013/HIEengage.pdf.
33. Meehan, R A., Staley, J. Facilitating Long-Term Care Providers’ Participation in Accountable Care Organizations through Health Information Exchange. Perspectives in Health Information Management. Summer 2017. Available at: https://perspectives.ahima.org/facilitatingltcproviders/.
34. Filipova, A. A. “Health Information Exchange Capabilities in Skilled Nursing Facilities.”
35. Rudin, R. S., A. Motala, C. L. Goldzweig, and P. G. Shekelle. “Usage and Effect of Health Information Exchange: A Systematic Review.”
36. Healthit.gov (May 2013). Governance Framework for Trusted Electronic Health Information Exchange | HealthIT.gov. [online] Available at: https://www.healthit.gov/sites/default/files/GovernanceFrameworkTrustedEHIE_Final.pdf
37. Ibid An Evaluation of Hospital Information Systems Integration Approaches. Available at: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.712.42&rep=rep1&type=pdf
38. An Evaluation of Hospital Information Systems Integration Approaches. Available at: http://citeseerx.ist.psu.edu/viewdoc/download?doi=10.1.1.712.42&rep=rep1&type=pdf