
Medication Management Technologies for Long-Term and Post-Acute Care: A Primer and Provider Selection Guide
Contents
1. Purpose of the Whitepaper, Executive Summary, and Disclaimer
1.1. Purpose of the Whitepaper
1.2. Executive Summary
1.3. Disclaimers
2. Definition of Medication Management Process
3. Problems Associated with Medication Management
3.1. Medication Errors
3.2. Adverse Drug Events
3.3. Use of Potentially Inappropriate Drugs for Older Adults
3.4. Polypharmacy
3.5. Transitions of Care
3.6. Medication Non-Adherence
3.7. Increased Resource Utilization
4. Medication Management Strategies
4.1. Medication Therapy Review and Reduction of Medications
4.2. Medication Therapy Management
4.3. Medication Reconciliation at Transitions of Care
4.4. Education, Medication Self-Management, and Adherence
4.5. Role of Clinicians and Other Professionals
5. Types and Uses of Available Medication Management Technologies
5.1. Upstream Technologies
5.2. Order Communications Technologies
5.3. Downstream Technologies
6. Benefits of Different Medication Management Technologies
6.1. Medication Errors/Adverse Drug Events
6.2. Medication Adherence
6.3. Hospitalization and Hospital Readmissions
6.4. Financial Outcomes
7. Potential LTPAC Provider Business Models
7.1. Medicare/Medicaid
7.2. Medicaid Waiver
7.3. Potential Affordable Care Act (ACA) Related Opportunities
7.4. Private Insurance
7.5. Standard of Care and Other Payment Sources
7.6. Return on Investment (ROI) of Medication Management Technologies
7.6.1. ROI to Patients and/or their Families
7.6.2. ROI to Payers
7.6.3. ROI to Care Providers
7.6.4 Online ROI Calculator
8. Planning for and Selecting Appropriate Medication Management Solutions
8.1. Visioning and Strategic Planning
8.1.1. Vision
8.1.2. Strategic Plan
8.2. Operational Planning
8.2.1. Project Team
8.2.2. Assessment Phase
8.2.3. Goal Setting
8.2.4. Program Design
8.2.5. Technology Review and Selection
8.2.6. Implementation Phase
8.2.7. Post-Implementation Phase
9. Selection Matrix Elements
10. Acknowledgement of Contributors
10.1. Contributing Writers
10.2. Workgroup Members
10.3. Participating Medication Management Solutions Vendors
11. References and Resources
1. Purpose of the Whitepaper, Executive Summary, and Disclaimer
1.1 Purpose of the Whitepaper
The purpose of this paper is to aid LeadingAge and other aging-services organizations in understanding the range of medication management technologies available in the marketplace, their uses, and the benefits of their use. The paper will also include a link to a matrix comparing existing medication management solutions that will help providers select solutions that best fit their requirements.
1.2 Executive Summary
This paper begins by defining medication management and its different phases, then outlines some of the issues related to medication management commonly experienced by older adults in a variety of care settings.
The whitepaper then provides an overview of the different medication strategies utilized throughout the medication management phases to mitigate these issues and discusses the potential role for various medication management technologies, citing evidence of efficacy or cost effectiveness where found.
Learn about medication management; find technology to help.
Potential long-term and post-acute care (LTPAC) provider business models including Medicare, Medicaid, Medicaid Waiver, and private insurance coverage are explained in section 7. In addition, this section provides an overview of potential Affordable Care Act (ACA)-related opportunities. Finally, this section concludes with a discussion about return on investment (ROI) for medication management.
Section 8 reviews the planning process for medication management solutions. It helps organizations prepare through visioning and strategic planning, looking at organizational readiness, operational planning, and technology review and selection, which walks providers through the must-have attributes, functionalities, and features they need to consider before using the CAST Medication Management Technology Selection Matrix and Online Selection Tool.
The whitepaper concludes with a description of the components of the CAST Medication Management Technology Selection Matrix, which is included in section 9. This matrix compares commercially available products from vendors who agreed to participate and provide information across hundreds of functionalities and features including fit for certain care settings.
Key information from the CAST Medication Management Technology Selection Matrix was included in an online Medication Management Technology Selection Tool. This tool helps LTPAC organizations narrow their selections. As an organization answers key questions, the tool creates a manageable list of products that meet the organization’s business line, care applicability needs, and essential requirements.
1.3 Disclaimers
This information is meant to assist in understanding medication management technologies, but it cannot possibly include all systems that may be available. Products mentioned in this report are only illustrative examples, and LeadingAge or LeadingAge CAST have not tested, independently evaluated, or endorsed them.
Please use this document as a general guideline to see examples of current medication management systems and to see how they work. Where appropriate, we identify provider case studies.
2. Definition of Medication Management Process
Medication management is a process that aims to facilitate safe and effective use of medications. This process involves several phases:
- Prescribing in the outpatient setting or ordering in the hospital and long-term care settings.
- Order communication, including transmission and verification.
- Dispensing and administration.1
Medication prescribing or ordering involves selecting a medication from the pharmacy benefit list and obtaining appropriate dispensing authorization. Order communication involves the clinician transmitting a prescription or order, and the pharmacist’s subsequent review and approval of this transmission. Medication dispensing and administration involve providing a supply of medication to an individual for whom it is ordered, giving the prescribed dosage to the patient, and documenting the medication administration.2
Upstream vs. Downstream
The prescribing or ordering phase is often referred to as upstream while dispensing, taking, or administering the medications is referred to as downstream. While each phase of medication management can introduce problems, existing and emerging technologies can address some of them.
3. Problems Associated with Medication Management
Problems associated with medication management can vary based on the care setting. Someone in the home can face different issues than someone living in a skilled nursing facility. Yet common threads appear in most care settings.
Older Adults and Persons with Disabilities at Risk
Older adults and persons with disabilities are generally more likely to suffer from multiple chronic conditions, to have multiple health care providers, to experience decreased cognition, and to transition among multiple care settings. As a result, these populations have more challenges with medication management.
For example, as the number of chronic conditions or the severity of disability increases, the number of prescribed medications, each with its own medication regimen, often rises as well.3
Below are the most common medication management issues that older adults face.
3.1. Medication Errors
Medication errors involve provision of the wrong medication, dosage, or route and can occur at the prescribing, dispensing, and administration phases of medication management.4
3.2. Adverse Drug Events
Adverse drug events (ADEs) are injuries (physical or mental harm or loss of function) resulting from the medication errors and can occur in any phase of the medication management process. Medication errors such as unfavorable drug-drug interactions and drug allergies can lead to ADEs.5
Older adults experience a disproportionate share of unwanted and unexpected adverse effects from medication. Falls, hip fractures, delirium, and urticaria lead the list of preventable adverse drug events. About 1 in 3 older persons taking at least 5 medications will experience an adverse drug event each year, and about two thirds of these patients will require medical attention.
ADEs Are Dangerous — and Preventable
Approximately 95% of these reactions are predictable, and about 28% are preventable.6 Adverse drug events due to errors, prescribing, administering, or non-adherence are defined as preventable.
ADEs are the sixth leading cause of death among hospital patients.
In Hospitals
According to a recent review,7 ADEs are the 6th leading cause of mortality among hospital patients, with 400,000 preventable ADEs estimated to occur in hospitals each year.
The notion of preventable ADE-related mortality is not limited to the hospital setting: 800,000 preventable ADEs are estimated to occur each year in nursing homes, and 530,000 among Medicare beneficiaries in outpatient clinics.8
In Nursing Homes
Approximately one in seven nursing home residents with an ADE requires hospitalization, underscoring the connection between medication errors and care transitions among older adults.9 A more recent study found that an estimated 22% of Medicare beneficiaries experienced adverse events during their skilled nursing facility (SNF) stays.
An additional 11% of Medicare beneficiaries experienced temporary harm events during their SNF stays. Physician reviewers determined that 59 percent of these adverse events and temporary harm events were clearly or likely preventable. They attributed much of the preventable harm to substandard treatment, inadequate resident monitoring, and failure or delay of necessary care.
More than half of the residents who experienced harm returned to a hospital for treatment, with an estimated cost to Medicare of $208 million in August 2011. This amount equates to $2.8 billion spent on hospital treatment for harm caused in SNFs in FY 2011.
The study used a 2-stage medical record review to identify events for a sample of 653 Medicare beneficiaries discharged from hospitals to SNFs for post-acute care. Sample beneficiaries had SNF stays of 35 days or less.10
At Home
Finally, medication errors and ADEs can also occur in home health care settings, especially as the number of medications increases.
3.3. Use of Potentially Inappropriate Drugs for Older Adults
Older adults are also more likely to take a medication that has been prescribed inappropriately — one that’s unnecessary, ineffective, or potentially dangerous — and to suffer an ADE. In a study of more than 150,000 older adult patients, 29% had received at least one of 33 potentially inappropriate medications.
A study of approximately 27,600 Medicare patients documented more than 1,500 ADEs in a single year.11
Tools Like Beers List, STOP, and START can reduce the risk.
Several tools can help clinicians lower older adults’ use of inappropriate medications, including these:
- Beers Criteria: Beers List is the most commonly used tool. First released in 1991, it is routinely updated with new medications and studies on medication safety. The Beers List was initially created to help clinicians determine which medications to avoid in nursing homes, as these patients are particularly at risk for medication-related problems.12
- STOPP Criteria – Screening Tool of Older Peoples Potentially Inappropriate Prescriptions: STOPP includes 65 clinically significant criteria that can help flag inappropriate prescribing in older adults. Each criterion is accompanied by a concise explanation as to why the prescribing practice is potentially inappropriate.
- START Criteria – Screening Tool to Alert Doctors to Right Treatments: Used in conjunction with STOPP, START consists of 22 evidence-based prescribing indicators for diseases commonly encountered in older people.13
- ARMOR – Assess, Review, Minimize, Optimize, and Reassess: This tool was created to consolidate these recommendations into an interactive functional tool. It takes into account the patient’s clinical profile and functional status, and it tries to balance evidence-based practice with altered physiological reserves. ARMOR is an effort to approach prescribing medications for older adults with multiple chronic conditions and comorbidities in a systematic and organized fashion. It aspires to restore and maintain a patient’s functional status. This tool also emphasizes quality of life as a key factor for making decisions on changing or discontinuing medications.14
3.4. Polypharmacy
Aging involves progressive impairments in the functional reserve of multiple organs, which might also affect drug metabolism and pharmacokinetics. In addition, older adults tend to develop multiple diseases, including multiple chronic conditions, and often take several medications concurrently. This scenario is called polypharmacy.15
Taking multiple medications increases risk.
Polypharmacy is problematic when patients are prescribed too many medications, since the higher the number of medications a patient takes, the higher the risk of medication errors, drug interactions, and adverse reactions. This risk is especially high for people with cognitive impairment who often forget to take their medications as prescribed.16
Polypharmacy is also associated with side effects such as increased risk of falls, dementia, and urinary incontinence, in addition to potential drug-drug complications and ADEs. Polypharmacy becomes especially problematic when the multiple medications are prescribed by multiple healthcare providers working independently of each other who do not know the patient’s complete medication regimens.17
Further, if patients use multiple pharmacies, individual providers and pharmacies are unlikely to have comprehensive, up-to-date information about the patients’ current medications or medication histories. This fragmentation of medication information can increase the risk of medication errors and ADEs.18
Over the counter (OTC) medications, herbals, and supplements add to the polypharmacy of prescribed medications and are usually harder to track and address.
3.5. Transitions of Care
Transitions in care are defined as the movement of patients from one health care practitioner or care setting to another as the patients’ condition and care needs change.
During these transitions, patients are much more susceptible to medication errors and medication-related problems due to many factors. These include medication changes, complex medication regimens, and incomplete handoff of information between the many caregivers and health professionals involved in the patient’s care.
Medication errors not only increase the possibility of causing patient harm, but also lead to substantial increases in healthcare utilization and costs.19
Multiple Settings and Fragmented Care
Institutions often function in isolation, despite the fact that collaboration across healthcare institutions is central to effective care transitions.20
Receiving care in multiple care settings creates fragmentation. Care is not coordinated, which can cause competing plans of care, duplication of services, medication errors, and patient confusion.
Half of all medication errors stem from poor communication.
Experience from hundreds of organizations has shown that poor communication of medical information at transition points, particularly information about medications, causes as many as 50 percent of all medication errors and up to 20% of adverse drug events in the hospital.21
Each time a patient moves from one care setting to another where orders change or must be renewed, clinicians should review previous medication orders alongside new orders and plans for care, then reconcile any differences.
No single longitudinal electronic patient health information across all settings of care exists, which complicates the issue.
Older Adults and Frequent Transitions
Older adults and those with disabilities who are served by long-term and post-acute care may use medications in multiple care settings, including their own homes, hospitals, assisted living facilities, and nursing homes, and they may experience frequent transitions across these care settings.
Medication management problems can occur in all care settings and in all phases of the medication management process. For example, medication errors and ADEs can occur with prescribing/ordering medications in nursing homes, hospitals, home health care settings, and assisted living facilities.
The patchwork of settings that serve older adults and people with disabilities can introduce additional medication management challenges. When patients transition across care settings, critical health information — including information about medications, drug allergies, and co-morbidities — is not always effectively communicated. Communication breakdowns raise the risk of medication errors and ADEs.22
Moreover, a patient’s medication schedule is often different before acute care and after transitioning to a new care setting. Some changes are related to the problem that caused the hospitalization; others simply relate to differences in formularies used in hospitals vs. long-term and community-based care settings.
There are 2 pertinent questions regarding medications for each care setting:
- How was the patient’s medication history and current regimen communicated during the transition to the present site of care?
- Given that all medications are ultimately the responsibility of the patient’s attending physician, how is that physician engaged in medication management? The answer depends on the setting in which the prescriber is practicing:
- Ambulatory – Physician office – managing patient residing in “community setting”: Office-based primary care physicians (PCP) managing the cognitively intact populations are the least restrictive. Some PCP groups include pharmacists as members of the clinical team.
- Long-term Care (LTC) – Skilled nursing facility (SNF), nursing facility (NF), assisted living facility (ALF), dementia care, and homebound: These locations have the most unstable and complex patient population and the least sophisticated strategy. The three primary provider groups serving each patient are facility staff, attending physician (on-site or office based), and LTC specialty pharmacy. Each has to answer to a federal, state, and/or third-party regulatory environment that is not aware of the other parties’ regulations. This setup creates a discontinuous care model that runs counter to the best interest of all parties.
3.6. Medication Non-Adherence
Medication adherence is defined as the extent to which patients take medications as prescribed by their health-care providers.23
Lack of patient adherence contributes to medication errors, with one study finding that 21 percent of errors in older adults were related to medication non-adherence.24
The Role Patients Play
Although ADEs are closely connected with provider behavior, patients also have a critical role in medication management. Non-adherence to medication regimens is a major cause of nursing home placement of frail older adults. For many, the ability to remain independent in their homes depends on the patients’ and/ or caregivers’ ability to manage a complicated medication regimen.25
Quantifying medication adherence among older adults and people with disabilities is challenging, as standard definitions and approaches to detection and reporting are lacking. Currently, self-reporting is the most common approach to ascertaining medication adherence, although this method is often unreliable.26
75% of Americans report not taking their medicine as prescribed.
Nonetheless, a survey by the National Community Pharmacists Association found that approximately 75 percent of American consumers report not taking their medicine as prescribed.27
It is reasonable to speculate that, as age and the number of medical conditions and medications increase, and as cognitive function decreases, the accuracy of self-reported medication adherence information may decrease. Indeed, one meta-analysis reported medication adherence rates among adults age 65 and older ranging from 26 to 59 percent.28
While medication non-adherence can result from patients’ choice not to follow their health care providers’ advice, it is also caused by patients’ inability to comply for a variety of reasons. Whether by choice or not, medication non-adherence is a challenging issue among older adults and people with disabilities.
This important aspect of medication management is related to the dispensing and administration phases, and it is most relevant to outpatients.
Reasons for Non-Adherence
Reasons for non-adherence vary, but the most widely mentioned include the following:
- Cost of certain medications.
- Lack of funds for filling the prescription.
- Lack of transportation to the pharmacy.
- Lack of medication knowledge (why they are taking the medication and the consequences of missing doses).
- Poor vision (unable to read the label).
- Physical dexterity (unable to open the bottle).
- Cognition (forgetful).
Knowing the predictors of poor adherence can help identify patients who need individualized medication strategies. It also can inform global health interventions to improve adherence.29
Possible interventions for increasing adherence include the following:
- Providing relief for prescription cost, providing low-cost insurance, and providing drugs to patients who cannot afford them.
- Providing home delivery of medications.
- Educating patients, a key driver for medication adherence.
- Modifying the container label, providing pill boxes, and using blister packs instead of childproof containers for older adults.
- Providing reminders for patients to take their medications, such as memory cues, electronic personal reminder systems, pill boxes, and telephone call programs, as well as associating medication taking with certain routine activities, such as a meal or bedtime.
3.7. Increased Resource Utilization
Every year, nearly one in five Medicare patients discharged from the hospital is readmitted within 30 days. Many policymakers view this costly reality as a symptom of a failing U.S. health care system.30
Discharge planning with medication management at the core is essential for reducing emergency room visits and hospital readmissions.
Discharge plans with medication management instructions can reduce hospital readmissions.
The Centers for Medicare and Medicaid Services (CMS) estimates that 11% of hospital readmissions occur due to medication non-adherence, creating an economic impact that is estimated to cost nearly $100 billion annually.31
Medication-related adverse events are a leading cause of injuries resulting in trips to the emergency room and hospital admissions.
4. Medication Management Strategies
4.1 Medication Therapy Review and Reduction of Medications
A comprehensive medication therapy review (MTR) occurs when a health care professional, such as a pharmacist or physician, thoroughly evaluates a patient’s medication regimen. The goal is to promote positive outcomes and minimize adverse consequences from medication.
The review includes but is not limited to preventing, identifying, reporting, and resolving medication-related problems, medication errors, or other irregularities. It also involves collaborating with other members of an interdisciplinary team.32
It is considered the first step in a successful medication management program, especially for older adults with multiple chronic conditions and multiple care providers in any care setting.
Medication therapy review (MTR) promotes positive outcomes.
Such reviews can help address polypharmacy and the problems associated with inappropriate medications. A number of technologies can facilitate them.
According to the nursing facility regulations and interpretive guidelines found in Appendix PP of the Centers for Medicare and Medicaid Services (CMS) State Operations Manual (SOM), consultant pharmacists are federally mandated to perform monthly medication regimen review.33
MTR Technologies
The range of technologies that facilitate MTR include the following:
- Interoperable electronic health records (EHR).
- Electronic prescribing (ePrescribing).
- Computerized physician order entry (CPOE).
- Clinical decision support systems (CDSS).
- Health information exchange (HIE).
- Software designed to help consulting pharmacists conduct these reviews.
Some of these technologies embed and implement automated alerts based on Beers list,34 STOPP and START criteria,35 ARMOR tool 36 and others that have been developed to reduce the potential of using inappropriate medications, as mentioned in section 3.2.
Pharmacist and Team Reviews
Studies have found that pharmacist-led medication reviews can correct some medication-related discrepancies, lower medication costs, and decrease the number of drugs prescribed.37 For example, an 8-month prospective trial of an active medication review by a pharmacist was carried out on 330 residents in nursing homes.
The number of drugs prescribed in the intervention group fell, but not in the control group. Overall, the clinical medication review reduced the number of medications prescribed with minimal impact on morbidity or mortality.38
A team approach that educates the health care professional and patient, where feasible, is effective in decreasing the number of medications taken by older patients and reducing adverse drug events. Assessment teams involving pharmacists and nurses can evaluate drug regimens and suggest changes.
Occasionally, pharmacists will conduct stand-alone medication brown-bag reviews and suggest changes. Serious consideration of these changes may help preempt adverse drug events.
Also, recent advances in technology, including mobile devices and computerized alerts associated with an electronic health record, can reduce adverse events.39
Computer monitoring systems can prevent 28% to 95% of ADEs.
Computer monitoring systems that reduce medication errors can prevent anywhere from 28 percent to 95 percent of ADEs. Computerized medication order entry has the potential to prevent an estimated 84 percent of dose, frequency, and route errors.40
4.2. Medication Therapy Management
Medication therapy management (MTM) is medical care provided by pharmacists whose aim is to optimize drug therapy and improve therapeutic outcomes for patients. Eleven national pharmacy organizations adopted this definition in 2004.
Pharmacists provide medication therapy management (MTM).
Medication therapy management is broader than medication therapy review and includes a range of professional activities, including but not limited to the following:
- Performing patient assessment and/or a comprehensive medication review.
- Formulating a medication treatment plan.
- Monitoring efficacy and safety of medication therapy.
- Enhancing medication adherence through patient empowerment and education.
- Documenting and communicating MTM services to prescribers in order to maintain comprehensive patient care.
The Five Components
Medication therapy management includes five core components:
- A comprehensive medication therapy review (MTR).
- Personal medication record (PMR).
- Medication-related action plan (MAP).
- Intervention and/or referral.
- Documentation and follow-up.
An MTR is a systematic process of collecting patient and medication-related information that occurs during the pharmacist-patient encounter. In addition, the MTR assists in identifying and prioritizing medication-related problems. During the MTM encounter, the pharmacist develops a PMR for the patient. The PMR includes all prescription and nonprescription products and requires updating as necessary.
MAP: A Plan for the Patient
After assessing and identifying medication-related problems, the pharmacist develops a patient-specific MAP. The MAP is a list of self-management actions necessary to achieve the patient’s specific health goals. In addition, the patient and pharmacist utilize the MAP to record actions and track progress towards health goals.
During the MTM session, the pharmacist identifies medication-related problem(s) and determines appropriate intervention(s) for resolution. Often, the pharmacist collaborates with other health care professionals to resolve the identified problem(s). Following the patient encounter and/or intervention, the pharmacist must document his/her encounter and determine appropriate patient follow-up.41 MTM has been shown to have a potential to positively influence medication adherence and prescribing quality. 42 43
Medication therapy management is a unique niche for the pharmacy profession, allowing pharmacists to apply their extensive knowledge as medication experts with the intent of improving patient outcomes. The Medicare Modernization Act of 2003 has required Medicare Part D prescription drug plans to include medication therapy management services delivered by a qualified healthcare professional, including pharmacists, since 2006.44
In 2010, CMS made the requirements for the MTM services more specific to promote consistency in this program. The program now targets beneficiaries who meet these guidelines:
- Have at least two or three chronic conditions (such as diabetes, asthma, hypertension, hyperlipidemia, and congestive heart failure),
- Take two to eight covered Part D medications, or
- Are likely to incur annual costs above $3,000 for all covered drugs.
In addition, all plans were required to enroll eligible beneficiaries in the MTM program exclusively using the opt-out method. Finally, CMS required MTM programs to offer a comprehensive medication review (CMR) for all of its beneficiaries annually, with additional quarterly targeted medical reviews (TMRs). On a prescriber level, sponsors are required to offer interventions to beneficiaries’ prescribers (e.g., physicians or nurse practitioners) to resolve medication-related problems.45
Best Practices for MTM
A recent comprehensive review of MTM services provided under Medicare Part D revealed wide variations in program design and efficacy for different disease conditions, etc. However, the review showed an effective MTM program includes the following practices:46
- Establishing proactive and persistent comprehensive medication review (CMR) recruitment efforts.
- Targeting and aggressively recruiting patients to complete a CMR based on two elements: information on medical events such as recent a hospital discharge, plus a scan for the usual MTM eligibility criteria.
- Coordinating care by utilizing trusted community relationships including networks of community pharmacists to recruit MTM eligible candidates, and utilizing existing working relationships between MTM providers (pharmacists) and prescribers to make recommendations and discuss identified problems for patients.
- Employing intensive patient education efforts aimed at addressing adherence barriers, including communicating to the patient a comprehensive understanding of each medication’s importance.
- Documenting the opportunities that were addressed with the patient for switching to generics or formulary alternatives.
- Improving drug adherence by providing a complete list of prescribed medicines.
- Addressing financial barriers to adherence such as high drug costs by potentially switching to generics or less-expensive formulary alternatives.
- Documenting the quality and safety of prescribing as part of the MTM intervention record (e.g., angiotensin-converting-enzyme inhibitors (ACEi) or angiotensin II receptor blockers (ARBs ) in congestive heart failure (CHF) and diabetes, cardio-selective beta-blockers in CHF, drug-drug interactions, high-risk medications).
- Conducting follow-up, documentation, and resolution of any identified drug safety issues.
- Using efficient communication methods to convey medication recommendations to prescribers, including the use of ePrescribing and electronic medical records.
- Leveraging all available data sources (EHR, registries, claims data) to determine whether gaps in medical care are present, including preventive care and maintenance care related to the patient’s specific medical conditions (e.g., HbA1c and screening for kidney damage in diabetes patients).
MMT Technologies
The range of technologies that facilitate MMT include the following:
- Interoperable electronic health records (EHR).
- Electronic prescribing.
- Computerized physician order entry (CPOE).
- Clinical decision support systems (CDSS).
- Health information exchange (HIE) and registries, including immunization registries.
- Software designed to help consulting pharmacists conduct such therapy management.
Some of these technologies embed and implement automated alerts based on Beers list,47 STOPP and START 48 criteria, ARMOR tool 49 and others that have been developed to reduce the potential of using inappropriate medications, as mentioned in section 3.2.
4.3. Medication Reconciliation at Transitions of Care
Medication reconciliation involves a systematic and comprehensive review of a patient’s medication regimen at the point of transition in care.50 The process then entails creating the most accurate list possible of all medications a patient is taking—including drug name, dosage, frequency, and route—and comparing that list against the physician’s admission, transfer and/or discharge orders.
The goal: Correct medications at all transition points.
The goal is to give the patient correct medications at all transition points.51 If this process does not occur in a standardized manner that is designed to ensure complete reconciliation, based on complete and up-to-date information, medication errors may lead to adverse events and harm.
Key Elements of the Medication Reconciliation Process
- Is fully electronic and automated.
- Employs a standardized process across all care settings.
- Supports a multidisciplinary, team approach.
- Employs a single list, used by all clinicians within a care setting, to document and validate a patient’s current medications upon admission.
- Features electronic access to the patient’s medication information from various sources, including community pharmacies, physician offices, and past medical records.
- Is fully integrated into the clinician’s workflow with effective prompts, reminders and/or forcing functions. These functions automatically populate the patient’s electronic medical record.
- Is fully integrated into the management of the patient’s medication regimens and is not considered to be an “additional task.”
- Features advanced clinical decision support that integrates documented care plans with the patient’s current medication regimen, compares this information to the medications ordered during the episode of care, electronically identifies unintended discrepancies, and alerts the clinician to those discrepancies.
- Includes electronic capabilities to assist the clinician with auto-substitution upon admission, based on formulary implications.
- Sends messages directly to physician pagers or inboxes when updates or changes to the patient’s home medication list occur and/or when discrepancies are identified and require clarification.
- Has an electronic, seamless process to communicate medication lists—as well as changes to that list—to the next provider(s) of service.
- Makes sure patients and/or caregivers are active participants in the medication reconciliation process.
A toolkit from the Agency for Healthcare Research and Quality (AHRQ) suggests that an ideal medication reconciliation process encompasses the following:
The AHRQ toolkit is based on the Medications at Transitions and Clinical Handoffs (MATCH) program developed at Northwest Memorial Hospital in Chicago with AHRQ support. The toolkit provides a step-by-step guide to improving the medication reconciliation process and incorporates the lessons learned by health care facilities that have implemented the MATCH strategies. While the toolkit is based on processes developed in acute-care settings, it can be adapted for use in post-acute facilities, according to AHRQ .52
A number of technologies facilitate the medication reconciliation process, including interoperable EHRs, electronic prescribing, computerized physician order entry (CPOE), clinical decision support systems (CDSS), health information exchange (HIE), and software designed to help clinicians conduct medication reconciliation.
4.4. Education, Medication Self-Management, and Adherence
Studies have found more than 50 percent of older adults knew the names and purposes of their medications; however, less than 25 percent knew the consequences of drug omission or toxic side effects.53 For example, one study of elderly patients with congestive heart failure found that 30 days after a new medication was prescribed, only 64 percent of the patients could identify when they were supposed to take their medicine.54
Older adults require specific educational methods.
Also, older adults were found to have insufficient knowledge of inhaler technique and to not understand how medications can improve their asthma.55 Patient education is a key intervention to assist older adults with medication management. Patient knowledge of drugs is positively associated with adherence.56
Education Geared to Older Adults
However, older adults require specific educational methods. Learning is more effective in older adults if information is explicit, organized in lists, and in logical order.
Instructions that are compatible with the older adults’ schema for taking medications are better remembered, and well-organized prescription labels are more useful for older adults.57 Studies have demonstrated that patient education and counseling over several home visits or with follow-up phone calls increased patients’ medication adherence.58
While traditional patient education provides information and technical skills, self-management teaches problem-solving skills.59 The growing emphasis on self-management recognizes that the patient plays a central role in preventing and managing illness.
For example, a self-management program for 489 chronically ill Kaiser Permanente patients resulted in improved health behaviors and health status.60 Furthermore, growing evidence from controlled trials suggests that self-management approaches are more effective than information-only education in improving clinical outcomes.
These approaches may also reduce costs and may soon become an integral part of high-quality primary care.61
Interventions to Improve Adherence
Additional possible interventions for improving adherence include the following, as outlined in section 3.5:
- Providing relief for prescription cost, providing low cost insurance, and providing drugs to patients who cannot afford them.
- Providing home delivery of medications.
- Educating patients and caregivers, a key driver for medication adherence that can be incorporated in MTR sessions, MTM, and medication reconciliation.
- Modifying the container label, providing pill boxes, and using blister packs instead of childproof containers for older adults.
- Providing reminders for patients to take their medications, such as memory cues, electronic personal reminder systems, pill boxes, and telephone call programs, as well as associating medication taking with certain routine activities, such as a meal or bedtime.
A number of technologies facilitate medication adherence, including alerts from the pharmacy when a prescription is not picked up; refill reminders; special packaging to facilitate recognizing, reading or opening medications; medication organizers; personal medication reminders; and personal medication dispensers.
4.5. Role of Clinicians and Other Professionals
Communication and collaboration among the different clinicians involved in providing care for older adults — including physicians, pharmacists (including clinical and consulting pharmacists), nurses, and case managers — is critical at all phases of medication management.
It is important to establish communication channels, processes, and collaboration protocols among everyone involved:
- Among all clinicians.
- Between the clinicians and the older adult and any family members who are invested in the success of the medication management program.
Technology can support clinicians and enhance collaboration by facilitating communication, making pertinent information available to all team members, and providing automated checks, alerts, and reminders.
5. Types and Uses of Available Medication Management Technologies
5.1. Upstream Technologies
Together, certain systems can reduce medication errors and ADEs associated with the prescribing/ordering and communication phases of medication management:
- Electronic Health Record (EHR): The EHR has been defined as a longitudinal electronic record of patient health information generated by one or more encounters in any care delivery setting.62 A patient’s medications, allergies, and problems are included in this information.
- Electronic Prescribing (ePrescribing): This technology is computer-based support for writing and transmitting prescriptions between a prescriber and a dispenser or pharmacy.
- Computerized Physician Order Entry (CPOE): CPOE is a computer-based system that automates a clinician’s process for entering orders, including medication orders, and transmits them to laboratories, nursing homes, and pharmacies.
- Clinical Decision Support Systems (CDSS): A CDSS has interactive software designed to assist physicians and other health care professionals with decision-making tasks such as determining patient diagnoses and issuing warnings. CDSS systems link health observations with health knowledge in ways that help clinicians provide improved care.63
Upstream technologies improve prescribing, ordering, and communication.
Upstream technology solutions, including health information technologies like EHRs with ePrescribing and CPOE functionality as well as CDSS, have the potential to reduce medication errors and ADEs associated with both prescribing/ordering medications and communicating medication orders.
Safety Risks
However, certain CPOE-related practices can create safety risks. For example, partial adoption of CPOE, or a lack of CPOE monitoring (e.g., incomplete data entry or excessive use of free text), can create hazardous conditions. Substantial evidence suggests that well-designed decision support not only enhances the quality of care, but also directly improves patient safety by decreasing common errors and preventing omissions or missed opportunities that harm patients.
In spite of this, many EHRs do not have robust or reliable decision support features, and poorly implemented IT systems have been shown to introduce errors that adversely affect care.64
Software-aided medication review protocols used by home health agencies also facilitate collaboration with pharmacists and physicians to reduce the risk of medication errors.
Using clinical information (medication use, vital signs, and other clinical indicators) collected and entered into a risk-assessment software system, users are alerted to potential medication problems determined by preset criteria.
According to protocol, nurses and care managers consult with pharmacists to verify the accuracy and appropriateness of the patient’s medication list and to identify potential problems that warrant reevaluation by a physician.65
5.2. Order Communications Technologies
Order communications technologies encompass the communications and messaging standards that the EHR, ePrescribing, or CPOE software utilizes to electronically communicate prescriptions or medication orders to the pharmacy and/or other health information technology systems.
These technologies allow different health IT platforms to communicate.
These technologies allow different health information technology platforms — including physician, LTPAC, hospital and pharmacy EHR systems, prescription drug plan databases, and stand-alone systems — to interoperate.
Today there are several standards that support interoperability and health information exchange either through a 1-to-1 exchange or one-to-many exchange mediated by a health information exchange (HIE) entity or a regional health information organization (RHIO).
These standards include a family of NCPDP Script Standards.
CMS Requirements
As of Nov. 1 2013, CMS required all Medicare Part D prescription and medication orders communicated electronically to use NCPDP SCRIPT version 10.6 or higher, with the exception of long-term care settings. Since NCPDP SCRIPT 10.6 or higher can handle three-way ePrescribing practices followed in some long-term and post-acute care settings, these settings were required to use this standard effective Nov. 1, 2014.
Now, LTPAC settings who choose to send Medicare Part D prescription or medication order information electronically to a pharmacy that is a separate legal entity from the one generating the prescription/ medication order must use NCPDP SCRIPT version 10.6 or higher. However, ePrescribing is still voluntary in LTPAC settings.
As of Jan. 1, 2012, CMS ePrescribing program for Medicare Part D requires the following:
- Accredited Standards Committee X12N 270/271-Health Care Eligibility Benefit Inquiry and Response, Version 5010.
- NCPDP Telecommunication Standard Specification, Version D.0 for eligibility queries between dispensers and Part D sponsors (i.e., prescription drug benefits insurance plans).
Finally, CMS requires DEA (Drug Enforcement Agency) EPCS (ePrescribing of Controlled Substances) application. 66 The SCRIPT Implementation Recommendations Document contains guidance for the use of one of the DEA options in SCRIPT v10.6. 67 All states except Montana and Missouri allow EPCS,68 and New York is mandating it effective March 27, 2016 (please see the extension of the effective date).
Other states may follow suit. However, providers implementing ePrescribing must ensure compliance with pertinent state regulations. This requirement includes any rules issued by their State Board of Pharmacies, particularly those related to prescriber’s signature and prescription of controlled substances, if applicable.
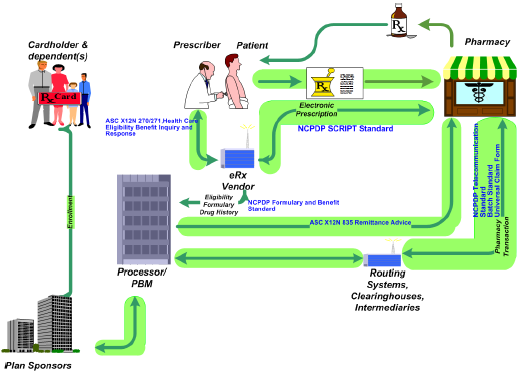
Figure 1. Current Communication Standards Used among Different Stakeholders of ePrescribing in Ambulatory Care Settings (Credit NCPDP)
During these communications, providers can get all medications that other providers prescribed to the patient. The pharmacy or insurer’s system may check eligibility, communicate co-payments, and/or suggest formulary alternatives to the prescriber or the pharmacy. Figure 1 depicts the different current standards used in communication between different stakeholders in ePrescribing in ambulatory care settings.69
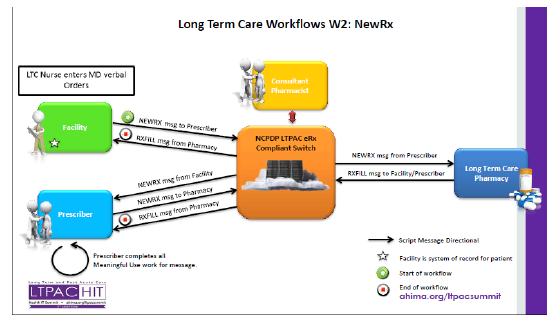
Figure 1. Current Communication Standards Used among Different Stakeholders of ePrescribing in Ambulatory Care Settings (Credit NCPDP).
Figure 2. Messages Exchanged and Workflows in Three-way ePrescribing in Long-Term Care Settings (Credit: Rod Baird and Shelly Spiro).
Downstream, electronic medication administration records (eMAR), bar-coded point-of-care systems, and remote pharmacy systems can reduce medication errors during medication administration in nursing homes, assisted living, and hospital settings.
Further, software-based screening protocols and pharmacists’ medication reviews can improve appropriate use and reduce potential for errors.70
Downstream technologies can improve medication administration accuracy and timeliness.
In the home, medication reminder, dispensing, and monitoring systems can reduce the non-adherence that can ultimately lead to ADEs in this care setting.
Telepharmacy
Telepharmacy facilitates access to medications and drug education for people who live in rural areas and those without easy access to traditional pharmacy services. Telepharmacy capitalizes on electronic information and telecommunications (telephone, fax machine, computer, internet, and video) to provide long-distance pharmacy services and support.71
Often, a registered pharmacist technician delivers medications to customers after a pharmacist working from a remote or central pharmacy processes and verifies the prescription. Pharmacists with access to EHRs can check prescriptions for dosing, allergies, duplication, and drug interactions.
Electronic dispensing of medications in rural hospitals facilitates administration of appropriate dosages and timing of medications.72 In this setting, telepharmacy can utilize automatic dispensing devices (ADD) that release prepackaged medications the pharmacist has authorized. Pharmacists can monitor the verification process, oversee restocking of the ADD, and use a videoconferencing link to counsel patients about their medications.73
Electronic Medication Administration Records (eMAR)
Health care professionals and clinicians use eMAR systems to manage workflow by documenting administration times for electronically ordered medications. These systems record patient medication, dose, and timing information, as well as special administration instructions.
Nurses use eMAR systems to document medication administration and reasons for non-administration. The systems generate alerts to prevent the wrong medication from being administered, prevent medication from being administered to the wrong person, and provide alerts when medications are overdue.
Finally, they store medication-related activities, generating a medication record for each patient.74
Bar Codes
Bar-coded medication administration (BCMA) combines eMAR with bar-coding equipment and software to ensure accurate medication administration and reduce medication errors at the point of care. Similar to the CPOE systems, the level of initial investment for BCMA can be significant.
Personal Medication Management Devices
Medication reminders, medication dispensers, and devices that combine informing, reminding, and dispensing functions are patient-focused technologies that aim to improve medication adherence. Most often, older adults and people with disabilities who live in the community, as well as people in service-enriched congregate settings such as assisted living facilities, use these devices.
The devices can be stand-alone or integrated into larger systems. Stand-alone technologies can provide single or multiple functions, and they may have advanced functions, including monitoring and data transmission.
Personal devices help patients take their medications properly and can improve adherence.
A single function medication dispensing system is easiest to use and least expensive, but it has limited functionality by design. Multi-function systems seek to enhance medication adherence using two or more functions.
Advanced technologies address one or more medication adherence elements, such as medication ingestion, metabolism, and adjustment, but are more complicated to use.
Recently, medication dispensers and reminders have been integrated with health-management capabilities, such as monitoring of overall health and storage of health information. These devices may offer broader self-management opportunities for older adults and people with disabilities.75
Medication reminders are devices that prompt patients to take their medications using audible or visual cues or both. The complexity of these devices ranges from wrist-watch alarms that generate alerts at various times to programmable computer software that informs users when it is time to take their medications.76 Because they are portable, some medication reminder devices can be incorporated into a person’s daily routine with relative ease.
Some devices combine a reminder technology with an automated dispenser that releases medication at specific times or intervals the user specifies.77 While some of these devices dispense only one medication, others can dispense multiple medications and/or handle varying schedules.
Medication dispensers often lack portability and require a standard electric outlet for reliable functioning. Nonetheless, they are appealing to both older adults and people with disabilities because these groups frequently have difficulty opening medication bottles and handling and sorting small pills. These dispensers mean patients need to handle medication containers less often, ultimately making the medication easier to take.78
The most advanced consumer-targeted technologies are devices that combine medication reminding, dispensing, and monitoring. These systems remind the user to take the medication, dispense the medication, and facilitate monitoring of when and in what quantities the medication was taken.
For example, some devices ask the user to log the date and time when the medication was taken while others collect and store this information automatically. Some of these devices can also report this information to the clinician and/or caregivers using internet, telephone, or text messaging.
This information allows caregivers to monitor how well patients are adhering to their medication regimens and take action when problems occur. Medication reminder and dispenser systems can cost up to $1,000, and the caregiver notification function can cost an additional $10 to $50 per month.79
6. Benefits of Different Medication Management Technologies
6.1 Medication Errors/Adverse Drug Events
ePrescribing and CPOE functionalities within an EHR can improve prescribing and ordering by catching errors at the point of care and reducing communication errors due to illegible handwritten prescriptions. They also can catch miscommunication between physicians and pharmacists.80
These systems give providers access to patients’ health records, including existing medications, medication history, drug allergies, and other information. The increased access to patient information these systems offer not only yields safer prescribing practices, but also can facilitate eligibility and formulary checks.
ePrescribing and CPOE become increasingly beneficial when used in combination with advanced features such as CDSS that provide real-time feedback to help prevent medication-related problems.
This type of support may involve patient-specific alerts that include information about allergies, drug interactions, medication history, pharmacy eligibility, drug coverage, formulary composition, other benefits, and any necessary dosage adjustments.81
CDSS with four key features improved clinical practice.
Key Features of CDSS
CPOE and CDSS vary in both complexity and capability. A review showed that 68% of CDSS implementation studies indicated improvement in clinical practice, including drug dosing and preventive care. The review identified these as the most important features of CDSS systems:
- Automatically providing decision support as part of clinician workflow.
- Giving decision support at the time and location of decision-making.
- Providing a recommendation.
- Using a computer to generate decision support.
Nearly all systems that had these four features (94%) improved clinical practice, compared to systems that had none of these features (46%).82
Research on ePrescribing and COPE with CDSS Capabilities
Published research has examined how ePrescribing systems operating independently and CPOEs that interface with CDSS affect medication errors and ADEs. These reports, which focus primarily on academic hospitals, suggest that CPOEs and CDSS systems reduce medication errors.
A recent review of the literature on ePrescribing assessed medication errors and ADEs in the outpatient, inpatient, and intensive care settings and found a significant risk reduction in all three settings. However, the magnitude of risk reduction varied by care setting, study design, sample size, and duration of follow-up.
This review also showed that custom-designed systems developed within an organization showed greater declines in medication errors than commercial systems, and systems with advanced CDSS showed greater benefit than did those with limited or no CDSS.
Despite these findings, the authors cautioned that more randomized controlled trials were needed to solidify the evidence base supporting the benefits of these technologies.83
CPOE can substantially lower medication errors in inpatient acute-care settings.
A more recent comprehensive systematic literature review derived a summary estimate of the effect of CPOE on medication errors. The estimate was combined with EHR adoption data from the 2006 American Society of Health-System Pharmacists Annual Survey, the 2007 American Hospital Association Annual Survey, and the latter’s 2008 Electronic Health Record Adoption Database supplement. Its goal was to estimate the percentage and absolute reduction in medication errors attributable to CPOE.
The study showed that processing a prescription drug order through a CPOE system decreases the likelihood of error on that order by 48% (95% CI 41% to 55%). Given this effect size, and the degree of CPOE adoption and use in hospitals in 2008, we estimate a 12.5% reduction in medication errors, or approximately 17.4 million medication errors averted in the United States in one year.
The findings suggest that CPOE can substantially reduce the frequency of medication errors in inpatient acute-care settings.84
Computerized prescribing alerts can reduce use of potentially inappropriate medications that could lead to ADEs. A 5-year study of computerized decision support tools found that drug-specific alerts in a community practice setting reduced the use of potentially inappropriate medications in patients age 65 and older.85
Another study found that CPOE systems have been shown to reduce 55% of serious medication errors and 17% of adverse drug reactions, leading to reductions of $500,000 in pharmacy charges and $26 per emergency visit.86
CDSS can improve prescribing and lower costs in nursing homes.
One of the few studies conducted in long-term care settings involved evaluation of a clinical event monitor to detect ADEs in nursing homes. It suggested that ADEs can be detected with a high degree of accuracy in this setting. 87
Another study demonstrated that computerized CDSS for physicians improved the quality of prescribing for nursing-home residents with renal insufficiency.88
As for potential cost savings, another study, which focused on long-term care facilities, found that CDSS for medication ordering reduced costs by $1,391.43, a 7.6% net reduction.89
Few studies have evaluated telepharmacy, and most published reports on this topic are pilot demonstrations that describe telepharmacy services and quantify the number of prescription consultations and costs. However, there has been some suggestion that telepharmacy offers promise for improving medication management.
A survey of state rural health offices found reductions in hospital medication error rates following implementation of telepharmacy.90
Benefits of Bar Codes
Evidence supporting the benefit of bar-coding and eMAR in hospitals is limited, with few rigorous studies examining health outcomes.91
Similarly, there have been few controlled trials of bar-coding and eMAR in nursing homes.92
Bar codes could prevent 95,000 potential ADEs related to medication administration each year.
Among published studies addressing outcomes associated with bar-coding and/or eMAR systems, a hospital-based study found that implementation of bar-coded medication verification technology embedded in an eMAR was associated with a 41% reduction in incorrect dosing and a 51% reduction in potential ADEs associated with those errors.
This report also showed a 27% decrease in errors associated with the timing of medication administration. Based on these findings, it has been estimated that BCMA could prevent approximately 95,000 potential ADEs each year at the point of medication administration, as well as an additional 50,000 potential ADEs related to transcription errors.93
Another study reported a 71% decrease in medication errors when nurses used bar-codes in a point-of-care information system. However, in this study, the bar-coding device was frequently avoided for several reasons, including lack of coordination among nursing staff and physicians, plus increased prioritization of monitored activities during busy periods.94
Thus, although there is some evidence to suggest that these technologies may reduce medication errors, important issues related to training and workflow may also need to be addressed to realize the full potential of these technologies. No peer-reviewed studies assessing the efficacy of bar-coding and eMAR in nursing-home settings have been identified.
6.2. Medication Adherence
Although there are only a limited number of rigorous studies evaluating medication reminder, dispenser, and monitoring devices, there is some evidence that they improve medication adherence. One study randomized 139 patients into three groups:
- A control group that did not receive any alerts/reminders.
- An intervention group that used medication bottles that remind patients to take their medication through audio and visual alerts and generate missed-dose reminder telephone calls.
- An intervention-plus group that received the alerts and reminders as well as a financial incentive.
After 6 months in the program, a preliminary analysis of this ongoing randomized trial found increased medication adherence among those receiving alerts/reminders, but no additional benefit associated with the financial incentive.
Interim results showed 98% medication adherence among the intervention group, 99% adherence among the intervention-plus group, and 71% adherence for those who did not use the reminder-generating bottles.95
Alerts, financial incentives, and medication dispensers can increase adherence.
6.3. Hospitalization and Hospital Readmissions
One study investigated the effects of three medication management approaches on adherence and resource utilization in older adults:
- A pillbox.
- A voice-reminder medication dispenser.
- Usual self-administration.
Patients using the medication dispenser were significantly more adherent than were those using a pillbox and those who self-administered their medications. Moreover, the group that self-administered its medications had more physician office visits and hospitalizations.96
Another study comparing automated medication dispensers to pillboxes in patients age 60 and older showed lower rates of hospitalization and emergency room visits among those using the medication dispenser.97
6.4. Financial Outcomes
Even though CPOE systems may require a significant up-front investment depending on individual providers’ characteristics and needs, it has been reported that improved communication, charge capture, and immediate response to laboratory results can generate substantial savings.
For example, one hospital in Massachusetts spent nearly $12 million to develop, implement, and operate a CPOE system between 1993 and 2002. This facility achieved a budget savings of nearly $10 million over the same time period.98
The CPOE system saved $10 million in one hospital, and a custom Bar Code systems realized positive ROI after 4.5 years in another.
The initial investment for BCMA also can be significant. For instance, the five-year cost for a custom-designed BCMA system at one hospital was $2.24 million, including planning, development, and rollout ($1.31 million), as well as $342,000 in annual operating costs.
Nevertheless, this system surpassed the break-even point and generated positive financial returns on investment within 4.5 years of full implementation.99
7. Potential LTPAC Provider Business Models
7.1 Medicare/Medicaid
Eligible professionals (EP), which include physicians, receive financial incentives from CMS under both the Medicare and Medicaid programs to use certified EHR technology (CEHRT) that have ePrescribing and/or CPOE capabilities.
Physicians and nurse practitioners (under the Medicaid program) practicing in LTPAC may choose to assign their incentive payments to their employer or entity with which the EP has a contractual arrangement in exchange for making certified EHR technology (CEHRT) available to them.
Under Medicaid, EPs also can choose to assign their incentive payments to their employer or to other state-designated entities. For more information please see the CMS EHR Incentive Program website and the Frequently Asked Questions on the EHR Incentive Program.
MTM Services Covered by Medicare and Medicaid
In addition, Medicare Part D Prescription Drug benefit and Part D plan sponsors cover MTM services by pharmacists or other healthcare professionals for eligible beneficiaries. These services include the following:
- Annual comprehensive medication review for all beneficiaries.
- Quarterly targeted medication review for select beneficiaries.
- Interventions by a prescriber (physician or nurse practitioner/ physician assistant) to resolve medication issues.
At least 20 states have Medicaid MTM programs with different eligibility criteria and at different stages of implementation.
7.2. Medicaid Waiver
Medicaid waivers are vehicles states can use to test new or existing ways to deliver and pay for health care services in Medicaid and CHIP. There are four primary types of waivers and demonstration projects:
- Section 1115 Research & Demonstration Projects: States can apply for program flexibility to test new or existing approaches to financing and delivering Medicaid and CHIP.
- Section 1915(b) Managed Care Waivers: States can apply for waivers to provide services through managed care delivery systems or otherwise limit people’s choice of providers.
- Section 1915(c) Home and Community-Based Services Waivers: States can apply for waivers to provide long-term care services in home and community settings rather than institutional settings.
- Concurrent Section 1915(b) and 1915(c) Waivers: States can apply to simultaneously implement two types of waivers to provide a continuum of services to the elderly and people with disabilities, as long as all federal requirements for both programs are met.100
According to a CAST Analysis of Medicaid Waiver Programs, 16 states, including California, Colorado, Connecticut, Iowa, Kansas, Minnesota, New Hampshire, New Jersey, New York, Ohio, Pennsylvania, South Dakota, Utah, Vermont, Virginia, and Washington, reimburse for home medication management services, including reminder/ dispensing under sections 1915(b) and/or 1915(c).
The analysis showed that Pennsylvania has the most comprehensive coverage for aging services technologies in its telecare program, which includes home telehealth, activity/wellness monitoring, medication dispensing, and personal emergency response systems (PERS).101
Rates and requirements vary. For more details about the coverage of medication management and other aging services technology services in these states, please see CAST Analysis of State Payment for Aging Services Techonologies (AST) at LeadingAge.org/CAST_Reports_and_Whitepapers.aspx.
7.3. Potential Affordable Care Act (ACA) Opportunities
The Affordable Care Act (ACA) is shifting the health care system in the United States away from the traditional fee-for-services to a pay-for-performance system. This change is starting to eliminate the misalignment of incentives inherent in traditional Medicare, Medicaid, and private insurance programs.
There are many provisions and models in the ACA that would benefit from, provide opportunities to cover, and consequently encourage the adoption of medication management technologies and services.102
New Models
The act created the Center for Medicare and Medicaid Innovations (CMMI), which is tasked with exploring new care delivery and payment models and initiatives103 that do the following:
- Use more holistic, patient-centered and team-based approaches to chronic disease management and transitional care.
- Improve communication and care coordination between and among care providers.
- Improve care quality and population health while reducing growth in expenditures.
The Affordable Care Act emphasizes health information technology.
The act puts explicit emphasis on the use of health information technology (health IT), including telehealth and remote patient monitoring, in Health Homes for Enrollees with Chronic Conditions, the Independence at Home Demonstration, and the Use of Technology in New State Options for Long-Term Services and Supports.104
These initiatives include the following:
- Hospital Readmission Reduction Program (HRRP).105
- ACOs. 106
- Bundling of Payments models, of which the following two are relevant to LTPAC providers:107
- Retrospective Acute Hospital Stay plus Post-Acute Services.10
- Retrospective Post-Acute Care Only. 108
LTPAC providers bring a significant value for hospitals, physician groups, payers, and accountable care organization (ACO) partners by providing the following services:
- Rehabilitation and skilled nursing facilities that provide post-discharge/post-acute patient rehabilitation.
- Skilled nursing facilities, assisted living facilities, continuing care retirement communities, housing with services, and home health agencies that provide post-acute patient stabilization and sub-acute chronic disease management.
- Holistic person-centered care, including support services.
- Lower-cost care settings than hospitals.
These new care delivery and payment models will provide LTPAC providers utilizing technologies—like health IT, medication management and telehealth and remote patient monitoring technologies—with opportunities to derive revenues from strategic partners.
7.4. Private Insurance
According to a 2013 report from the Association of Health Insurance Plans (AHIP), at least 16 private health insurance plans offered and covered MTM services. The report described trends in the medication therapy management programs being conducted by America’s health insurance plans.
It also provided details about 16 companies’ MTM initiatives for a variety of patient populations.
Themes in MTM
The report identified three common themes that emerged from the review of health plans’ MTM initiatives:
- Advanced IT systems are enabling new strategies for care improvement and cost savings.
- MTM is helping achieve the goals of new care delivery models such as accountable care organizations (ACOs) and patient-centered medical homes (PCMHs).
- Pharmacists’ roles are expanding in new and innovative ways to deliver effective, evidence-based care.
In addition, the second chapter of the report provides a company-by-company compendium of MTM programs in operation today, including results of these programs whenever available.109
7.5 Standard of Care and Other Payment Sources
LTPAC and community health providers, special population agencies, self-pay and self-insured organizations, and others, especially not-for-profits, may offer an array of medication management services.
Grants may cover these services. Or the organization may absorb the cost, with different revenue sources, including charitable contributions, covering it.
7.6. Return on Investment (ROI) of Medication Management Technologies
Return on investment (ROI) represents the ratio of the net gains relative to the initial investment over a certain period of time. Subsequently, ROI can be expressed in the following equation:
![]()
As discussed above, medication management delivers various benefits, including potential financial savings to different stakeholders, including patients and/or their families, payers, care providers, etc.
However, the financial savings and ROI depend on a number of factors including the care delivery model, the payment/reimbursement model, the technology, and of course costs. The first and most important step in calculating ROI is to consider the different stakeholders, identify the investors, and calculate the gains and savings netted/accrued to each investing stakeholder under each particular care delivery and payment model.
When calculating ROI, one should only include the gains that accrued to that particular stakeholder minus all expenses relative to that stakeholder’s own investment/cost. Often the reduction of hospital days is erroneously included in the providers’ ROI, which is not true under the traditional fee-for-service reimbursement model and can be misleading; such a reduction usually accrues to the payer.
7.6.1. ROI to Patients and/or their Families
ROI to patients and/or their families can be calculated as follows:
![]()
For private pay patients and their families, for example, the potential financial gains of medication management are many:
- Prolonging independence by avoiding deterioration in health that may lead to disability and
- Avoiding the need to move into assisted living or skilled nursing facilities, which is significant.
- Savings in co-pays for unnecessary medications eliminated during drug reviews.
- Higher medication adherence.
- Reducing recurring hospital visits.
- A higher quality of life, which is difficult to quantify.
The patient’s/family’s expenses and investment are the monthly out-of-pocket cost of medication management services, plus any co-pay for the occasional physician office visit, lab tests, and prescriptions.
7.6.2. ROI to Payers
ROI to payers can be calculated as follows:
![]()
For dual Medicare and Medicaid eligible patients who are nursing home eligible, for example, the financial gains of home telehealth and remote patient monitoring under a Medicaid Waiver program that accrue to Medicaid, which would otherwise be liable for the costs of nursing home room and board costs, lie in remaining in their own home with home health, home care, and other supportive services.
Medicaid’s investment is the monthly rate of home medication management services and additional supportive services aimed at keeping the individual independent.
In this particular example there may be additional savings, like reductions in hospitalization and hospital readmission costs that accrue to Medicare, which is liable for and covers health care costs.
Consequently, such savings or gains should not be included in calculating Medicaid’s ROI, which is investing in the medication dispensers and supportive services in this case.
7.6.3. ROI to Care Providers
ROI to care providers can be calculated as follows:
![]()
The care provider who makes investments in information and communications technology infrastructure, including the medication management technology and the clinical and care services, may gain these benefits:
Lower costs in delivering the same services, including staff efficiencies and staff travel costs (if the payer covers the remote services, rather than just the in-person visit).
Higher reimbursements/payment from the payer or strategic partner in terms of incentive payments for avoiding more costly care settings, procedures, events, or penalties.
For example, an LTPAC provider partnering with a physician group ACO to manage a chronically ill patient population can potentially get a percentage of the incentives or shared savings payments the ACO receives from the payer for reducing hospitalizations and hospital readmissions. These amounts can be significant for certain populations.
LTPAC Provider
The LTPAC provider’s net gain is:
+ The sum of all gains accruing to the LTPAC provider in staff efficiencies, increased referrals from the ACO, traditional fee-for-service payments, and additional incentive payments received from the ACO
– Minus the costs of leasing the home medication dispensing equipment and actual costs of services
delivered.
Physician Group ACO
The physician group ACO’s ROI is:
+ The portion of the payer’s incentive payment that it gets to keep plus any additional fee-for-service payments due to more frequent office-based services
– Minus the actual costs of services it delivers (for example in medication reconciliation or care coordination), relative to the portion of incentives it passes through to the LTPAC provider.
In contrast, in a partnership between an LTPAC provider and hospital under the traditional fee-for-service model, for example, the LTPAC provider may help its hospital partners reduce 30-day readmission rates for pneumonia, congestive heart failure, and acute myocardial infarction (heart attack) patients, helping the hospital avoid Medicare’s payment penalties under the HRRP.
The hospital may contract with and pay the LTPAC provider a percentage of the penalties saved for delivering medication management program that lead to reducing 30-day readmissions for patients discharged from the hospital after being admitted for one of these three conditions.
LTPAC
The LTPAC’s net gain is
+ Again the sum of all gains accruing to the LTPAC provider in staff efficiencies, increased referrals from the hospital, traditional fee-for-service payments, and additional payments received from the hospital
– Minus the costs of leasing the medication dispensing equipment and actual costs of services delivered.
Hospital
The hospital’s ROI is
+ The portion of avoided penalties it gets to keep, plus any additional fee-for-service payments it gains for more referrals due to improved quality ratings
– Minus the actual costs of services it delivers, relative to the portion of avoided penalties it passed through to the LTPAC provider, plus any additional costs incurred for staff time in care coordination, medication reconciliation, or health information exchange, for example.
7.6.4 Online ROI Calculator
Once individual investors have been clearly identified, an estimate of the ROI to the different stakeholders can be calculated. The SCAN Foundation has recently published a white paper on making the business case for person-centered care with instructions for using an ROI calculator they developed.
This return on investment (ROI) calculator is designed to quantitatively assess the business case for person-centered care (PCC) programs that serve older adults with chronic conditions and functional limitations. PCC programs are ones where individuals’ values and preferences are elicited and, once expressed, guide all aspects of their health care, supporting their realistic health and life goals. This type of care is achieved through a collaborative relationship and decision-making process among the person, their chosen supports, and their medical and social service providers. As discussed in detail above, the business case for PCC involves weighing the costs of offering this approach to care against the benefits expressed in dollar terms. Benefits accrue principally in the form of avoided medical utilization, but also potentially in the form of higher revenues.
The ROI calculator has a number of practical features:
- Risk Stratification: The population that is suitable to receive PCC can be segmented into high and moderate risk categories. The ROI will be likely higher (i.e., a higher percentage) for the segment that is at higher risk for medical utilization. The calculator can show how limited the offering must be if a specific return were being sought. Potential Revenue from PCC: The calculator allows for PCC program offerings to incorporate possible revenue enhancements in addition to the more probable benefits resulting from reducing costs.
- Slider Bars: This feature allows the user to compute instantaneous “what-if” calculations by changing values of inputs and immediately viewing these new inputs’ influence on the ROI.
- Flexibility in Expressing Variables: All variables can be entered by the user in terms of their convenience – per person, per month, or per year. Hospital admissions, for example, are generally reported on an annual basis whereas encounters with a social worker or nurse practitioner are often expressed on a monthly basis. The calculator automatically converts rates and volumes, no matter how expressed, into a common per member per month (PMPM) measure.
- Scenarios: This feature allows ROI comparisons across different programs as well as varied constellations of input values. For example, the user can create optimistic and pessimistic scenarios and compare the results. Sometimes even the pessimistic scenario can yield an acceptable result for the ROI.
- Accounting for Uncertainty: Admittedly, some key determinants of the ROI are not known with certainty. Therefore, a “Monte Carlo” simulation that accounts for uncertainty with respect to the magnitudes of key variables is an optional part of the tool. This simulation recognizes this uncertainty and displays accordingly a reasonable range of results for the ROI rather than a single deterministic value. The tool also quantifies the strengths of the separate influences each variable has on the resulting ROI.
- Other Metric – Payback Period: In addition to the ROI result, the calculator displays the payback period – defined as the number of months the PCC program would need to operate (assuming a positive operating margin) for any initial investment to be recouped. This metric may be useful for programs involving substantial up-front launch costs.
- Threshold Analysis: The tool provides the ability to conduct threshold analysis, whereby the user can query the calculator on questions such as the following: What is the maximum amount that can be spent on PCC so that the program does not lose money? Or for a given cost of delivering PCC, how effective must it be in reducing certain events (e.g., hospital readmissions) in order to generate a required (hurdle) level of ROI?
To access the calculator tool, go to The SCAN Foundation.
8. Planning for and Selecting Appropriate Medication Management Solutions
Medication management is a complex process that has multiple phases and spans a number of providers. It requires coordination and collaboration with a number of clinical professionals, may involve a number of departments within the same organization, and entails collaboration with different stakeholders, including the patient and the patient’s family in some cases.
Planning for medication management technologies entails focusing on the care settings, issues, root causes, and more.
Initiating, expanding, or integrating medication management as a service is complex and begins with understanding the care settings; issues; root causes; stakeholders involved, including the patient population; and operating environment, including the states where the program will be implemented.
To plan for this initiative, these items must be considered in light of the organization’s strategic goals and vision for a medication management program.
The next step is evaluating operational readiness and conducting operational planning, followed by due diligence in selecting vendor partners with experience in strategic planning, program design, and ongoing program development.
8.1 Visioning and Strategic Planning
8.1.1. Vision
To succeed, the organization must first develop its vision for acquiring and employing a medication management system.
Organizations implement medication management technologies to create a patient-centric environment that is safe, efficient, and effective. Reducing the effects of polypharmacy, the administration of inappropriate drugs, medication errors, and adverse drug events (ADEs) are all essential outcomes of a medication management system.
The care settings range from institutional (nursing homes, assisted living) to community-based care (private home, senior housing, and adult day services). Moving to a patient-centered care environment will improve patient care, reduce medication errors, improve quality of medication management, improve decision making, and increase administrative efficiency.
Honing the Vision
The organization’s vision should incorporate the following:
- What problems are you are trying to resolve?
Examples include polypharmacy, administration of inappropriate drugs, AEDs, errors in transitions, medication non-adherence in independent or community living settings, or inefficiency of medication administration. - What are the care settings?
Different care settings (home, community, skilled nursing, assisted living, senior housing, etc.) require different strategies, solutions, and technologies. - What goals and drivers are moving you toward this decision?
The goals are directly related and closely tied to the problems identified above. Specific goals may include promoting quality, improving patient care, improving accuracy and efficiency of medication administration, and/or reducing care transitions and hospital readmissions. - How does this vision align with your business needs?
Does medication management technology support the business? Will the medication management system support the organization’s billing functions and manage the utilization of high-cost drugs? Does the medication management system integrate with third-party pharmacy vendors?
For example, a skilled nursing home might be part of a larger health system, and a decision is made to move away from the institutional pharmacy vendor to the corporate pharmacy servicing the rest of the system. The medication management system must be able to communicate with the corporate pharmacy.
- What population are you serving?
Different populations in a home/community environment will have different needs than those in an institutional setting.
- Does the vision include accommodating the “10 rights” of medication administration?
- Right Medication: Is this the right medication the provider ordered, and is it labeled?
- Right Does: How many milliliters, tables, or does are to be given?
- Right Time: What time of day should the medication be given, and when was it administered last?
- Right Route: Should the medication be given by mouth, feeding tube, or injection?
- Right Patient: Is the medication for this patient, or is it for someone else?
- Right Patient Education: Inform the patient of the medication being given and the desired effects and potential side effects.
- Right to Refuse: Verify that the patient understands the consequences for refusal, notify the physician, and document.
- Right Assessment: Assess the patient to insure the medication is safe and appropriate; if not, document and contact the ordering physician.
- Right Evaluation: After administration, assess the patient for adverse effects and medication effectiveness’ compare the patient’s pre- and post-administration condition and document.
- Right Documentation: In the patient’s chart, document the medication, dose, route, date, and time, then sign.
8.1.2 Strategic Plan
Management gathers the resources necessary to guarantee successful systems implementation through strategic planning and an implementation plan. Strategic initiatives are typically long-term in nature and can have a profound effect on the organization, positive and negative. They must align with the organization’s mission, vision, and values.
Top management must help form the strategic plan with a vision for the medication management program.
Risk is a component of strategic planning, and any plan must evaluate the internal and external environments, culture, workforce, current systems, competitors, regulations, community, suppliers, and partners.
Strategic planning requires top management to participate, as they are the decision makers and usually have a holistic perspective of the environment in which the organization operates. Significant resources in capital and people are needed, which would require the commitment of the entire organization. Strategic initiatives usually have an impact on interdepartmental operations, and the stakeholders must be fully identified.
The strategic planning process yields the implementation plan. The strategic plan tells you what you are going to do; the implementation plan is a roadmap that tells you how you will get there and who will help. System implementation includes several phases. A high-level example follows.
8.2. Operational Planning
8.2.1 Project Team
A wide array of project stakeholders is key to a successful medication management program. The most successful ones incorporate the program into the organization’s day-to-day operations so that all staff have some involvement.
Since medication management programs can span several care delivery systems, most staff will need to be involved, including executive leadership, clinical teams, pharmacists, operations and finance personnel, technical representatives, and marketing/business development staff.
Getting all of these groups on board with a clear set of goals, timelines, resource requirements, and deliverables will lead to success.
8.2.2. Assessment Phase
The assessment phase is to evaluate and understand business objectives and goals; evaluate customers’ needs, capabilities, and current processes; review IT infrastructure and support systems; and understand the functional and operational requirements.
It is time to clearly identify the key stakeholders, the business drivers, and any known risks. Developing a survey for stakeholders to express their needs is an optional step that can support the decision to move forward.
During this phase, the team will review the regulatory environment, identify the resources required, and develop the project budget. Finally, it evaluates the feasibility of pursuing the project.
8.2.3. Goal Setting
Defining the medication management program’s goals is critical to measure success. Each organization will have different ideas of what success looks like based on internal operations. Before starting a medication management program, the organization should set a clear series of goals and metrics.
Goals should be measurable and reported on routinely.
Keep in mind that goals should be measurable and routinely reported on within your operations. Goals must be SMART (Specific, Measurable, Attainable, Realistic and Trackable). Setting both short-term and long-term goals for the medication management program is highly recommended.
Medication management programs will naturally change and progress over time. Organizational goals set at the initiation of the program will likely be different six to 12 months after implementation. Medication management program goals should continuously be evaluated and updated as programs change.
It is also important to understand that a new program will have the ability to achieve several major goals during the program’s initial adoption.
Types of Goals
Goals for each organization should be unique and may incorporate ideas from the following categories:
Safety and Clinical Outcomes:
- Fewer medication errors.
- Improved mediation adherence.
- Reeducation in adverse drug effects.
- Improved control of chronic conditions.
- Fewer hospitalizations.
- Fewer hospital readmissions.
Satisfaction Outcomes:
- Improved patient/caregiver satisfaction scores.
- Improved provider satisfaction scores.
- Increased trust from the patient.
Operational Outcomes:
- Increased staff productivity/efficiencies.
- Positioning and market advantage.
- Improved communication.
Financial Outcomes:
- Fewer readmissions.
- Increased revenue.
- Increased productivity.
Be sure to define outcome measures that will help in evaluating the program’s short- and long-term success. After determining program goals, ensure that baseline data has been captured and discussed during medication management planning sessions. These goals and metrics should be periodically reviewed and updated throughout the planning and implementation process.
8.2.4. Program Design
Medication management programs should be designed with the organization’s short- and long-term goals in mind to help ensure success. Coordination, collaboration, and communication to enhance patient care and outcomes with other care providers should also influence the program design.
Each program’s design should always consider how to align objectives, strategies, and technical plans with care partners. Programs can use medication management technology and the EHR, in addition to any telehealth and remote patient monitoring solutions, as sources of information and to facilitate communications.
The organization’s short-term and long-term goals will guide program design.
Be sure to share experiences from similar organizations to help build a medication management program within the organization or to strengthen an existing one. Please see the series of companion case studies CAST is collecting.
8.2.4.1. Issues, Care Settings, and Patient Populations
At the earliest stages of planning, an organization should identify the issues it is trying to resolve (such as medication non-adherence); the care setting where the patient, resident, or client lives; and patient population the organization wants to reach.
The Issues
Section 3 of this white paper reviewed some of the most common problems associated with medication management for older adult populations, and section 4 reviewed medication management strategies to help address such problems. One should also consider the following issues and nuances:
Supplements and over-the-counter drugs are often left out of the medication record.
- Patient competencies vary; patients need to be able to understand, remember, and follow the instructions on the medication to achieve good adherence.
- Shorter stays in acute care settings create an added burden on LTPAC providers who are receiving the patients who require a higher level of care sooner.
- Care transitions between different care settings are uncoordinated among multiple providers; the pre-admission medication list, hospital stay medication list, and discharge medication list can be incomplete, redundant, or missing.
- Fragmentation means a patient’s or resident’s medication data can be found in any number of locations: hospital, physician office, pharmacy, pharmacy benefits manager (PBM). The data can also be in different formats, paper and electronic, making access and retrieval difficult. The lack of a single up-to-date medication list opens the door for errors.
- Lack of a longitudinal patient record is an important issue; today’s systems do not have the means to integrate the patient data with medication data. All patient episodes of care need to be reflected in the record: inpatient, outpatient, physician office, and home.
- Dietary supplements and over-the-counter drugs are not always considered to be medications and are left off the medication record.
- Hoarding of medications by home-based patients as well as taking expired medications can be a risk.
- Medication delivery in SNF and AL facilities can be inconsistent. Facilities tied to a corporate parent use the corporate pharmacy; stand-alone facilities use local pharmacies or other institutional pharmacies.
- Prescribing practices may be inconsistent; for example not everyone is familiar with Beers Criteria for medications that are inappropriate for older adults.
- Cost of implementing health IT is significant and is stretching organizational budgets. Additional funding sources, such as grants, often need to be identified. Lack of financial incentives and no reimbursement for using health information systems in these settings continue to be an issue for the LTPAC sector.
- Domain-specific IT and/or clinical expertise to implement medication management technologies is in short supply; organizations that have such resources internally are often stretched and handle many competing priorities.
The Care Setting
Considering the care setting where medication management technology will be employed is essential for a successful medication management program. One needs to consider the differences between the following long-term and post-acute care settings:
- Home and Community Settings – Home, Independent Living, PACE, Hospice, Adult Day Care: Home health care is a system of care provided by skilled practitioners to patients in their homes under a physician’s direction. Home health care services include nursing care; physical, occupational, and speech-language therapy; and medical social services.110
The goals of home health care services are to help individuals to improve function and live with greater independence; to promote their optimal level of well-being; and to help them remain at home, avoiding hospitalization or admission to long-term care institutions.111 Home health visits often uncover the patient’s medication risks.
States have different laws on who can give medications in assisted living.
- Assisted Living: Assisted living provides or coordinates 24-hour-awake oversight and services to meet residents’ individualized scheduled needs, based on the residents’ assessments and service plans and their unscheduled needs.112 State regulations are unique in defining medication assistance, including who can assist with medications, who can administer medications, and the extent of staff training, supervision, and licensure required.
- Consequently, assisted living services that are provided in the context of “medication assistance” vary. Fourteen states require a nurse to administer medications. Nursing assistants are allowed to administer medications in 32 states. New York and Kentucky require assisted living residents to self-administer their own medications, and Louisiana and Minnesota require assisted living residents who cannot self-administer their medications to contract with an outside source.113
- Skilled Nursing: Nursing homes, or skilled nursing facilities, provide round-the-clock nursing care and significant assistance with the activities of daily living (ADLs). Nursing homes have nursing staff on duty 24 hours a day to help individuals meet their daily physical, social, and psychological needs. A licensed physician supervises each resident’s care. Therapy, including speech, occupational, and physical therapy, is available for rehabilitation. Skilled nursing follows an institutional pharmacy model.
The Patient
Moreover, one needs to consider the following characteristics of the patient population, especially for issues related to adherence and solutions where the patient plays an active role in the program:
- The level of care and support these individuals need is a factor of frailty, functional abilities, chronic conditions, the number of medications taken, cognitive status, mobility, manual dexterity (which affects their ability to open medication bottles), mental health, smoking, alcohol use and substance abuse, availability of caregiver, and support services, to name a few.
- Demographic diversity, including education, may affect the level of self-management in general and understanding of medication instructions in particular. Other aspects include income, which affects the patient’s ability to buy their medication; ethnicity; and locale (urban, rural, or inner-city).
- The behavioral profile includes motivation and activation levels, and propensity to anxiety and depression.
As part of this process, ensure that there is a process to identify and enroll patients and gather their consents, especially for patient-facing programs. For such programs, it is also important to understand the patient’s abilities, as mentioned above, when selecting a technology solution.
When selecting a personal patient-facing medication adherence system or advising a consumer who is selecting one, keep several things in mind:
- Number of medications and complexity of schedule: Make sure the solution can accommodate all the user’s medications and scheduling requirements. Start by having the user’s physician review all medications to make sure they are all necessary. In many cases, this step may yield fewer medications and/or a simpler medication regimen.
- Patient’s needs and abilities: Consider the patient’s needs. Does he or she have a simple medications regimen that warrants a simple reminding system? Or does the patient have a more complex medication regimen that warrants a dispensing function? How critical it is for the caregiver to know if the patient is non-adherent?
- Ease of use, programming, and filling: Assess the device’s ease of use to ensure that the older adult will be able to use it on a regular basis. Can the person program and fill the device without assistance? Filling will usually involve packaging the medications as well as filling the device. Alternatively, can a family caregiver program and fill the device for the older adult? Or will the family need a professional caregiver to program and fill the device?
- Refilling and monitoring responsibility: Based on the ease of filling and programming, someone will need to determine who will be responsible for refilling the dispenser when the medications run out. Should the device have a refill request feature? If the device has a monitored medication adherence solution, consider who will be responsible for receiving the non-adherence alerts. What will the response protocol entail?
- Portability: Portability is necessary for active older adults who spend a lot of time outside their “home” or travel frequently. If portability is required, consider the average length of trips when evaluating the pill capacity of a portable medication dispenser.114
Finally, demonstrating the value of medication management and making sure that patients understand their care will be improved, not diminished, is at the heart of the consent process, if applicable.
8.2.4.2. Operating Model, Workflow, and Change Management
When a new medication management program is implemented, it does not just mean adding technology into an existing care model; on the contrary, care models themselves may change as a result of introducing medication management technology. This is particularly significant for the clinical care model.
Use the technology to change care delivery and workflows, inside and out.
Before starting any program, make sure that the new model of care is clearly defined and that staff have been prepared with training and support plans. To gain the most benefit out of medication management technology, ensure it is used as a tool for changing care delivery and workflows, both inside the organization and with outside partners, and not simply an add-on.
Adding medication management technology, or any other technology for that matter, without assessing and redesigning processes and workflows to take advantage of the technologies’ capabilities and efficiencies, will likely fail to produce the anticipated benefits.
8.2.4.3. Business Model: Expenses and Revenue Sources
Consider the care delivery and payment model(s) being proposed for the medication management program and associated services. Identify all expenses including infrastructure, connectivity, medication management system expenses, installation, troubleshooting, maintenance and support, change management, training, and clinical and pharmacist services and support.
Identify all the revenue sources (private pay, payer, strategic partner), and carefully calculate the organization’s ROI, as well as the other stakeholders’.
8.2.5. Technology Review and Selection
Once an organization has completed the visioning and strategic planning exercise, assessed organizational readiness, assembled the project team, set the project’s goals, and designed the program, then the team needs to develop a set of requirements.
These requirements enable the team to select the medication management technology solution that can help achieve the program’s goals and meet an organization’s needs.
Choosing the Requirements
Setting
These requirements include the care setting where the medication management solution is deployed (pharmacy, home health, skilled nursing facility, housing with services, community-based programs, etc.). Depending on which medication management issue an organization is interested in addressing and the medication management phase the issue spans, the applicable technology solution may be dramatically different.
If an organization is interested in the technologies that focus on the upstream phase of medication management like medication ordering or prescribing to reduce polypharmacy, for example, it can choose a solution for ordering/prescribing and/or communication.
An organization interested in the downstream phase, like increasing medication administration accuracy and reducing ADEs or patients’ adherence to medications, can choose a solution focusing on dispensing, medication administration, or adherence.
Functionalities
Another important selection factor includes the specific desired functionalities for drug therapy. These may include the following:
- Bi-directional ePrescribing (at the ordering phase).
- Compliance packaging (at dispensing).
- Robotic dispensing (at the pharmacy).
- Unit dispensing systems (at the facility).
- Electronic medication administration record (eMAR).
- Electronic treatment administration record (eTAR).
- Closed-loop medication verification in care settings where staff administer medications.
In addition, medication adherence functionalities are important factors for settings and situations where taking medications is the individual’s personal responsibility, such as in independent living or home and community-based programs.
Consider if adherence solutions beyond reminders and organizing pills are needed.
When considering a personal medication adherence solution, it is important to consider whether or not solutions that go beyond organizing pills and reminding are needed, such as monitoring capabilities, locked/tamper-proof compartment, and auto refill request capabilities as well as any special packaging.
Lastly, it is important to consider whether the medication management program needs CDSS capabilities and/or technologies to facilitate medication reconciliation or medication therapy management capabilities, as these constitute important functionalities and selection factors.
Integration with Other Systems
The medication management system’s ability to integrate with other technology platforms such as electronic health records (EHRs), telehealth devices, medication adherence monitoring dispensers, safety monitoring systems such as personal emergency response systems (PERS), and/or wellness, behavioral and activity monitoring systems, multi-site integration, as well as analytic tools can also be critical to providers.
Legal and Regulatory Requirements
Other important selection factors are legal and regulatory requirements, such as approval for ePrescribing or dispensing of controlled substances, Joint Commission Certification for certain settings, and whether the system has been reviewed by the U.S. Food and Drug Administration (FDA) as a medical device prior to marketing and approved, cleared, or exempt and listed.
Has the system been approved for ePrescribing, dispensing, or as a medical device?
For approved medical devices, FDA has approved a premarket approval (PMA) application prior to marketing and deemed them safe and effective. This approval process is generally reserved for high-risk medical devices, such as pacemakers, and involves a more rigorous premarket review than the premarket notification, also known as 510(k), pathway. However, most medication management devices are not subject to premarket approval.
Cleared medical devices are devices that FDA has determined to be substantially equivalent to another legally marketed device. A premarket notification, referred to as a 510(k), must be submitted to FDA for clearance. A 510(k) is most often submitted by the medical device manufacturer.
Finally, medical devices that do not require FDA review before the devices are marketed are considered “510(k) exempt.” These medical devices are mostly low-risk, Class I devices and some Class II devices that have been determined not to require a 510(k) to provide a reasonable assurance of safety and effectiveness.
Such devices are exempt from complying with premarket notification requirements subject to the limitations on exemptions; however, they are not exempt from certain general controls. For example, 510(k) exempt devices must meet the following criteria:
- Be suitable for their intended use.
- Be adequately packaged and properly labeled.
- Have establishment registration and device listing forms on file with FDA.
- Be manufactured under a quality system (with the exception of a small number of class I devices that are subject only to complaint files and general recordkeeping requirements).
A medical device is FDA listed if the firm that manufactures or distributes the medical device has successfully completed an online listing for the device through the FDA Unified Registration and Listing System (FURLS). FDA listing allows post-market monitoring and reporting of any arising safety issues.
HIPAA and HITECH
The two other important legal and regulatory requirements include compliance with the Health Insurance Portability and Accountability Act (HIPAA), which set national standards to protect individuals’ medical records and other protected personal health information (PHI), as well as the Health Information Technology for Economic and Health (HITECH) Act, which sets additional standards to demonstrate meaningful use of security technology to ensure the confidentiality, integrity, and availability of protected electronic medical records and electronic personal health information (ePHI).
Electronic health information exchange can facilitate care coordination, particularlty medication reconciliation.
Electronic health information exchange capabilities are gaining significant importance for purposes of care coordination, especially around shared care and transitions of care.
Certification provides added assurance of interoperability. Providers are encouraged to determine if they need a certified EHR, under the ONC-ATCB certification program, which is focused on Meaningful Use.
Hardware and Software Requirements
Finally, hardware and software requirements that could be important to the selection process include how the software is offered:
- As a local model, which means that it needs to be installed on servers local to the care provider.
- As third-party hosted/Software as a Service (SaaS) model, where the software is hosted somewhere else and the provider pays licensing and hosting fees or pays for usage, as opposed to maintaining local server infrastructure.
Other important hardware and software requirements include remote access functionality support, off-line functionality support (when running 3rd-party hosted or SaaS software) and mobile device support (such as on smartphones and tablets).
CAST Medication Management/EHR Online Selection Tools
The CAST Medication Management Online Selection Tool can narrow selections to a few shortlisted candidate systems and vendors that meet must-have high-level requirements. Please note that since some of the medication management functionalities, especially in the upstream ordering and prescribing and downstream medication administration by staff phases, are offered in electronic health records, providers interested in solutions for these phases are also encouraged to use theCAST EHR Online Selection Tool.
This recommendation applies to ordering and prescribing systems such as CPOE, ePrescribing, CDSS, and Medication Reconciliation capabilities and administration functionalities such as eMAR/eTAR, and Closed Loop Verification.
The CAST Online Selection Tools help providers create a shortlist of vendors.
Please note one vendor may not provide the best fit medication management solutions for issues that span multiple phases. Organizations may need to use the online selection tool multiple times to identify potential solution elements for the different phases, then integrate into a best-of-breed solution for the comprehensive program.
In these cases, interconnectivity, interoperability, and/or system integration are especially important. Working with third-party system integrators and implementing integration engines for the different technology components of the comprehensive medication management program may be best.
Selection Matrix and RFP
The CAST Medication Management Selection Matrix outlines many additional options and detailed features and functionalities that will help drill down into these shortlisted products and narrow the selection to a list of two to four vendors that can be invited to submit request for proposals (RFP).
During the RFP process, providers are encouraged to interview prospective vendors, engage front staff as well as pharmacists, nursing and medical directors, and representatives from management, finance and IT teams in the interviews and product evaluation.
Demo, Case Studies, and References
The best approach is to conduct a demonstration, score the product and demonstration performance objectively, check provider case studies with the vendors, including case studies collected by CAST, and conduct appropriate due diligence including reference checking.
In addition, LeadingAge members may want to use the LeadingAge CAST/Technology Listserv (subscription required) to ask peers about the shortlisted products and their experience with these vendors.
8.2.6. Implementation Phase
The implementation and planning phase takes the information gained by the assessment phase and begins to develop answers to the who, how, and when questions. During this phase, the members of the executive steering committee are identified and a project charter is created. Enough time should be set aside for this phase, as it is involved and detailed.
This stage includes agreeing upon project scope and goals, developing a communication plan, and identifying the project team members who will actually implement the system. The project implementation team should be a patient-centered interdisciplinary team consisting of at a minimum physicians, nurses, pharmacists, IT staff, and, if appropriate, residents/patients, and families. A project plan identifying milestones, resources, tasks, and timeline comes from this phase.
The focus should include the patient’s journey through care settings.
Project tasks include mapping clinical and business processes and developing new processes and procedures. The scope should not be confined to the medication management processes. Prescribing, dispensing, and medication reconciliation are important processes, but the implementation team is patient-centered, so the focus should include the patient’s journey. The patient’s journey through care settings needs to be part of the mapping; otherwise the system will focus on medication ordering and dispensing.
Contingency planning is part of the overall plan; the team must assess and identify potential risks throughout the project and deal with them quickly. Most often, risk is not going to severely impact the project, but when a risk that could impact the project’s timeline, budget, or goals appears, the steering committee should be made aware to make decisions.
8.2.7. Post-Implementation Phase
Once the project is complete, monitoring and evaluation are important functions to see if the critical success factors were achieved to create a safe, effective, and efficient patient-centered environment. The transfer of knowledge from the implementation team to those who will be using the system is critical for the system’s sustainability.
Refresher training and an internal user group ensure that users are aware of the system’s new features and functionality as they are developed. A clinical and financial analysis should be done post implementation to see if the goals of the project were attained.
9. Selection Matrix Elements
CAST’s Medication Management workgroup, consisting of providers, vendors, and consultants, compiled a list of medication management products that serve the LTPAC market, as well as a list of functionalities and capabilities that would help providers choose the medication management product that best fits their business line and functional requirements.
Each medication management vendor was then provided the opportunity to complete a self-review of the workgroup’s pre-determined questions. Some of these vendors chose not to participate. Those who did participate were then invited to nominate a case study from a provider’s perspective on the use of the vendor’s medication management product.
The Medication Management Selection Matrix includes the following information:
Solution Applicability
Solution applicability illustrates the different medication management phase(s) to which a product is applicable, including the following:
- Ordering/Prescribing (Complete EHR, Computerized Physician Order Entry (CPOE) Software, E-Prescribing Software, Medication Management Clinical Decision Support System, Other).
- Order/Prescription Communication (Medication Order Management System, HIE-based Medication Management Clinical Decision Support System, Telepharmacy, Other) Dispensing Pharmacy (Pharmacist EHR, Consulting Pharmacist Software, Pharmacist Clinical Decision Support System, Pharmacy Management System, Compounding Software, Packaging, Robotic Dispensing and Carousels, Pharmacy Kiosk, Other).
- Administration to/Adherence of the Patient/Resident/Client (Medication Administration Verification Software (eMAR, eTAR, Closed-Loop Verification), Medication Reminder Systems, Personal Medication Dispenser, Other).
Business Line/Care Applicability
Business line/care applicability illustrates the various business lines to which the medication management product is applicable, including the following:
- Acute Care Settings (Physicians’ Offices, Emergency Department, Hospitals, Attending LTPAC Physician).
- Pharmacy Settings (LTPAC Pharmacy, Retail Pharmacy, Specialty Pharmacy, Consulting Pharmacy, Telepharmacy, Mail Order Pharmacy).
- LTPAC and Other Settings (Home Health/Home Care, Hospice, Housing with Services, Community Based Programs, Adult Day Care/Senior Centers, Assisted Living Facilities, Acute Rehab Facilities, Long-term Acute Care Hospitals, Long-term Care Rehab Facilities, Skilled Nursing Facilities, Intermediate Care Facilities, Intellectual Disabilities/Mental Retardation/Developmental Disabilities (ID/MR/DD) Facilities, Continuing Care Retirement Communities (CCRC), Program of All-Inclusive Care for the Elderly (PACE), Accountable Care Organizations (ACO)/Integrated Delivery Networks (IDN), Multiple Site Integration).
Ordering Functions Requirements
These requirements are the basic requirements that a user would look for when identifying a medication management system for ordering medications. They include the following:
| Admissions, Discharge and Transfers (ADT) | Substances or Yes; with Controlled Substances) | Medication Regimen Review (MRR) |
| Immunization Documentation | Medication Management Clinical Decision Support (Drug-Drug/ Drug-Allergy Interactions) | Medication Therapy Management (MTM) |
| Lists: Allergies | Insurance Coverage Check | Medication Reconciliation |
| Lists: Medications | Generic Alternative Check | Billing/ Claim Submission |
| Evaluation of Resident/ Client Signs and Symptoms | Reduction of Medications | Workflow Management/Next Step Prompts and Reminder |
| Computerized Physician Order Entry (CPOE) (In-Patient, Out-Patient, or Both) | Dose Reduction and Documentation | Analytic/Reporting Capabilities (e.g. Adverse Drug Event) |
| Bi-Directional ePrescribing (No, Yes; without Controlled | Frequency and Monitoring of Medications |
Pharmacy Functions Requirements
These requirements are the basic requirements to look for when identifying a medication management system for a pharmacy. They include the following:
| Admissions, Discharge and Transfers (ADT) | Evaluation of Resident/ Client Signs and Symptoms | Substances or Yes; with Controlled Substances) |
| Immunization Documentation | Computerized Physician Order Entry (CPOE) (In-Patient, Out-Patient, or Both) | Medication Management Clinical Decision Support (Drug-Drug/ Drug-Allergy Interactions) |
| Lists: Allergies | Bi-Directional ePrescribing (No, Yes; without Controlled | Insurance Coverage Check |
| Lists: Medications | Medication Regimen Review (MRR) | Workflow Management/Next Step Prompts and Reminder |
| Generic Alternative Check | Medication Therapy Management (MTM) | Analytic/Reporting Capabilities (e.g. Adverse Drug Event) |
| Reduction of Medications | Medication Reconciliation | |
| Dose Reduction and Documentation | Billing/Claim Submission | |
| Frequency and Monitoring of Medications |
Dispensing Function Requirements
These requirements are the basic functions a user would look for when identifying a medication management system for medication dispensing. They include the following:
| Compounding Software | Unit Robotic Dispensing (Stationary or Mobile) | Return to Stock |
| Automated Counting | Pharmacy Management System | Refill Management (Reminder) |
| Robotic Dispensing | Bar-Code Scanning | Interactive Voice Response (IVR) |
| Compliance Packaging (Commingled, Unit Packaging, or Both) | Rx Verification |
Administration Functional Requirements List
This list includes the following:
| Medication Organization | Closed-Loop Medication Verification | Administration Instructions |
| eMAR | Alerts and Reminder | Exception Documentation |
| eTAR | Next Step Prompts | Medication Error Tracking/ Reporting |
Personal Adherence Functional Requirements
These requirements include the following:
| Medication Organization | Dispensing Function | Maximum Numbers of Doses/Reminders Per Day |
| Medication Storage | Portable/Mobile Unit | Maximum Compartment Pill Capacity (if applicable) |
| Audio Reminder | Locking to Prevent Tampering | Special Packaging Required |
| Visual Reminder | Double-dose Prevention | Is a professional needed to create or change the programming? |
| Vibration Reminder | Required List: POTS, DSL, High-Speed Internet, WiFi, Cellular | PRN Monitoring/Tracking |
| Administration Instructions (audio, visual, both) | If Monitored, List Monthly Monitoring Fee | Remote Updates |
| Multi-Language Support (List Supported Languages) | Auto-Refill Request | Remote Configuration Capability |
| Is the Device Remotely Monitored? | Is a professional needed to refill? | |
| If Monitored, List type of Connectivity Supported/ |
Non-Adherence Alerts
This element addresses whether the non-adherence alerts can be sent to the following external parties:
- Client/Patient’s Physician
- Client/Patient’s Nurse/Other Licensed Clinician
- Client/Patient/User/Self
- Care Manager/Professional Caregiver
- Family
- Other
Non-adherence alerts also include the alert modality, which includes the following:
- Pager
- Telephone (Voice Messages)
- Text Message
- Other
Non-Adherence Reports and Personal Health Record (PHR)/EHR Access
This element includes whether the following reports/records can be:
- Customizable Reports
- Capable of Scheduling Automatic Reports
- Accessible by the following:
- Client/Patient’s Physician
- Client/Patient’s Nurse/Other Licensed Clinician
- Client/Patient/User/Self
- Care Manager/ Professional Caregiver
- Family and/or
- Other
Program Development and Support Offered
This category includes options for the following:
| Program Development (Planning, Business Model Templates, etc.) | Consulting Pharmacist Services | Patient Education |
| Pharmacy Services | Specialty Pharmacy Services | Patient Engagement |
| On-Site Pharmacy Services | Medication Reconciliation | Family Engagement |
| Telepharmacy Services | Billing Services (e.g., Medicare Part D) | Other |
| Mail-Order Pharmacy Services | Physician Engagement Services |
Hardware and Software Requirements – Front End
These requirements list the required desktop/laptop specifications for Software-Only Solutions, including requirements for the following:
- Minimum Processor Speed, Hard Drive Storage, RAM requirements if applicable.
- Operating System (OS) – Windows.
- Operating System (OS) – Apple.
- Operating System (OS) – Unix/Linux.
Other features compared include the following:
| Network Specifications | Miscellaneous Reporting Specifications (i.e., Crystal Reports) | Off-Line Functionality Support |
| Wireless Specifications | Scalability | Ability to Store/Handle Attachments (Insurance card, Historical Notes, etc.) |
| Modern Browser Support | Local Model | Available for Lease |
| Minimum Internet/Bandwidth Specifications | Hosted Model | Available for Purchase |
| Miscellaneous Software/Applets Needed (i.e., Citrix) | Software as a Service Model (SaaS) | |
| Remote Access |
Last, mobile options are listed as the following:
- Cellular Carriers that Support Solution.
- Mobile OS – Android.
- Mobile OS – Blackberry.
- Mobile OS – iOS.
- Mobile OS – Unix/Linux.
- Mobile OS – Windows.
- Mobile-Optimized Interface (through dedicated app or mobile-optimized web pages).
Finally, we added a tab for any Additional Notes on hardware and software requirements.
Interfacing, Integration, and Add-Ons
This section looks into the medication management solution’s integration capabilities with the following:
- Electronic Health Records (EHR).
- Patient/Family Portal.
- Medication Adherence Monitoring Dispensers.
- Biometric Telehealth/Telemonitoring Technologies.
- Safety Monitoring Systems such as Personal Emergency Response Systems (PERS).
- Wellness, Behavior, and Activity Monitoring Systems.
- Printing Support.
- Financial Software: Billing/AR/AP/General Ledger, etc.
- External Consulting Pharmacy and Medication Therapy Management Software (if applicable).
- Analytic Tools; Please list (e.g., Population Health Management and Adverse Event Reporting).
- Content/Document Management System/Devices.
- Other.
Interoperability, Interoperability Standards, and Certification
This section begins with type of interoperability and exchange capabilities supported, which includes the following:
- None, Export Data Only, Import Data Only, or Bi-Directional Data Import and Export
- Exchange Capability Supported (Direct, HIE/RHIO mediated, Both)
The section then lists a number of interoperability standards that the system may support, which includes the following:
- NCPDP 10.6 or Higher.
- EDI with Wholesalers.
- Blue Button Plus- Machine Readable.
- ICD-9 Diagnosis and Procedures: No, Yes (through billing clearinghouse), Yes (built in compatibility).
- ICD-10 Diagnosis and Procedures: No, Yes (through billing clearinghouse), Yes (built in compatibility).
- NDC – Medications (Manufacturers).
- RxNorm – Medications (Ordering).
- UNII – Allergies and Adverse Reactions.
- SNOMED CT – Reference Terminology for Clinical Data.
- IHE BPPC–Basic Patient Privacy Consent Profile.
- EDI HIPAA Profile/ File Formats (Please List).
- List Script Standard Versions Supported.
- Other.
The section ends with information on Back-End System Certification, which includes:
- 2014 ONC-ATCB Certification and whether it is:
- Complete (please provide link).
- Modular (please provide link).
- Not Certified.
- Plan on pursuing ONC’s proposed voluntary certification?
Program Support Services
This section includes options for the following:
- Equipment Delivery/Pick Up.
- Site/Home Installation.
- IT/Network Troubleshooting and Support.
- Front-End System Set-up/Programming.
- Front-End System Customization.
- Back-End System Set-up.
- Back-End System Customization.
- Onsite Staff Training.
- Online Staff Training.
- Onsite User/Patient Training.
- Online User/Patient Training.
- Equipment Cleaning.
- Equipment Refurbishing.
- Other.
Clinical Supportability
This area includes options for the following:
- Phone Support (No, Yes 24 hours, Yes limited hours).
- Web Support (No, Yes 24 hours, Yes limited hours).
- E-Mail Support.
- Listserv and/or Usergroup.
- Online Training.
- Onsite Training.
- Other.
Technical Supportability and Warranty Information
This section includes technical support options for the following:
- Phone Support (No, Yes 24 hours, Yes limited hours).
- Web Support (No, Yes 24 hours, Yes limited hours).
- E-Mail Support.
- Listserv and/or Usergroup.
- Online Training.
- Onsite Training.
- Other.
It also includes warranty options that include Length of Product Warranty and goes on to share what is covered under warranty:
- Parts.
- Parts and Labor.
- Parts and In-Field/On-Site Labor.
Legal/Regulatory/Cyberliability
This area touches on the following:
- FDA Clearance/ Listing – Cleared, Listed (this category may include Medical Device Data System (MDDS)), Pending, or None.
- FDA Classification (Class I, Class II, etc.).
- Pharmacy Systems Audited and Approved for ePrescribing Controlled Substances.
- Support of 340B Program.
- HITECH.
- HIPAA.
- E-Signature for Beneficiary.
- E-Signature for Authorized User.
- Security – List HIPAA & HITECH Act Requirements Met.
- Joint Commission Certification (If Yes; please list setting).
- List Applicable Regulatory Requirements Met.
- Provide a Link to Company’s Cyberliability Policy.
- List Any Other Legal Requirements.
- Provide Link to Sample Contract.
Hardware and Software Requirements – Back End
These requirements list the required desktop/laptop specifications for Software-Only Solutions, including requirements for the following:
- Minimum Processor Speed, Hard Drive Storage, RAM requirements if applicable.
- Operating System (OS) – Windows.
- Operating System (OS) – Apple.
- Operating System (OS) – Unix/Linux.
Other features compared include the following:
| Network Specifications | Miscellaneous Reporting Specifications (i.e., Crystal Reports) | Remote Access |
| Wireless Specifications | Scalability | Off-Line Functionality Support |
| Modern Browser Support | Local Model | Ability to Store/Handle Attachments (Insurance card, Historical Notes, etc.) |
| Minimum Internet/Bandwidth Specifications | Hosted Model | Available for Lease |
| Miscellaneous Software/Applets Needed (i.e., Citrix) | Software as a Service Model (SaaS) | Available for Purchase |
Last, mobile options are listed as the following:
- Cellular Carriers that Support Solution.
- Mobile OS – Android.
- Mobile OS – Blackberry.
- Mobile OS – iOS.
- Mobile OS – Unix/Linux.
- Mobile OS – Windows.
- Mobile-Optimized Interface (through dedicated app or mobile-optimized web pages).
Finally, we added a tab for any Additional Notes on hardware and software requirements.
Company’s Experience and Viability
This area includes the following:
- Number of Years in Business.
- Release Date of Current Version.
- Number of Patients Served.
- Core Customer Base/Focus of Line of Business.
- Links to Additional Case Studies.
The last section of the matrix is dedicated to the following:
- Strengths.
- Areas for Improvement.
- Ongoing Development.
- References.
10. Acknowledgement of Contributors
10.1. Contributing Writers
Majd Alwan, LeadingAge CAST
Rod Baird, GPM, LLC
Patrick Clark, St. Peter’s Health Partners, Trinity – Catholic Health East
Scott Code, LeadingAge CAST
10.2. Workgroup Members
Majd Alwan, LeadingAge CAST
Stephen Axelrod, TabSafe Medical Services Inc.
Rod Baird, GPM, LLC
Patrick Clark, St. Peter’s Health Partners, Trinity – Catholic Health East
Scott Code, LeadingAge CAST
Bob Davis, Optimus EMR
Donna Dulong, INRange Systems, Inc.
Craig Lehmann, Stony Brook University
Jim Pierce, Talyst
Shelly Spiro, Pharmacy HIT Collaborative
Sharon Thompson, Philips Home Healthcare
Anna Whitaker, HealthMEDX
10.3. Participating Medication Management Solutions Vendors
Twenty-four vendors, including 8 CAST Partners, Supporters and Business Associates, participated in developing the Medication Management Portfolio. These included:
- Philips Home Healthcare, a LeadingAge Silver Partner and CAST Supporter.
- PointClickCare, a LeadingAge Silver Partner with CAST Focus.
- MatrixCare, a LeadingAge Silver Partner with CAST Focus.
- Netsmart, CAST Supporter
CAST Business Associate participating in the portfolio included:
- Eldermark Software
- Health Care Software, Inc.
- LG CNS.
- Cantana Health (formerlly NTT Data LTC).
Other participating vendors included:
- ADL Data Systems
- American Data
- ClarityLife
- CompuMed
- gEHRiMed EHR
- Helix Pharmacy Management System
- LifeAssist
- MedReady
- RNA Pharmacy Solutions
- SigmaCare
- TabSafe Medication Management System
- Talyst
- Vorro Health
11. References and Resources
1. Agency for Healthcare Research and Quality (2010). Enabling medication management through health IT: Review protocol. Rockville, MD: U.S. Department of Health and Human Services. Available online at:https://www.ahrq.gov/prevention/guidelines/index.html. Last accessed July 11, 2014.
2. Agency for Healthcare Research and Quality (2010). Enabling medication management through health IT: Review protocol. Rockville, MD: U.S. Department of Health and Human Services. Available online at:https://www.ahrq.gov/prevention/guidelines/index.html. Last accessed July 11, 2014.
3. Murray, M.D., Morrow, D.G., Weiner, M., Clark, D.O., Tu, W., Deer, M.M., Brater, C, Weinberger, M. (2004). A conceptual framework to study medication adherence in older adults. American Journal of Geriatric Pharmacology, 2(1):36-41.
4. National Academy of Sciences (2007). Preventing medication errors: Quality chasm series. Available online at:https://www.nap.edu/catalog/11623. Last accessed July 11, 2014.
5. National Academy of Sciences (2007). Preventing medication errors: Quality chasm series. Available online at: https://www.nap.edu/catalog/11623. Last accessed July 11, 2014.
6. Pham, C.B., Dickman, R.L. (2007). Minimizing Adverse Drug Events in Older Patients. AmFam Physician, 76(12):1837-1844. Available online at: https://www.aafp.org/afp/2007/1215/p1837.html. Last accessed July 11, 2014.
7. Medication Management Chapter, Aging Services Technology Study: Report to Congress (2012). Available online at:https://aspe.hhs.gov/basic-report/report-congress-aging-services-technology-study. Last accessed July 14, 2014.
8. Institute of Medicine (2006). Medication errors injure 1.5 million people and cost billions of dollars annually. Available online at: http://www8.nationalacademies.org/onpinews/newsitem.aspx?RecordID=11623. Last accessed July 14, 2014.
9. Harjivan, C., Lyles, A. (2002). Improved medication use in long-term care: Building on the consultant pharmacist’s drug regimen review. The American Journal of Managed Care, 8(4), 318-326.
10. Adverse Events in Skilled Nursing Facilities: National Incidence among Medicare Beneficiaries. 2014. OIG Report OEI-06-11-00370. Available online at: http://oig.hhs.gov/oei/reports/oei-06-11-00370.pdf. Last accessed July 14, 2014.
11. Wooten J., Galavis J. (2005). Polypharmacy: Keeping the elderly safe. Available online at:http://www.modernmedicine.com/content/polypharmacy-keeping-elderly-safe. Last accessed Sept. 8, 2014.
12. American Society of Consultant Pharmacists. Available online at: https://www.ascp.com/articles/beers-list-criteria. Last accessed Sept. 8, 2014.
13. Gallagher, P., Ryan C., Byrne, S., Kennedy, J., O’Mahony, D. (2008). STOPP (Screening Tool of Older Persons’ Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther., 46(2):72-83. Available online at: https://www.ncbi.nlm.nih.gov/pubmed/18218287. Last accessed Sept. 8, 2014.
14. RazaHaque, M.D. (2009). ARMOR: A Tool to Evaluate Polypharmacy in Elderly Persons. Annals of Long-Term Care, 17(6). Available online at: https://www.managedhealthcareconnect.com/content/armor-a-tool-evaluate-polypharmacy-elderly-persons. Last accessed Sept. 5, 2014.
15. Klotz, U. (2009). Pharmacokinetics and drug metabolism in the elderly. Available online at:https://www.ncbi.nlm.nih.gov/pubmed/19514965. Last accessed Sept. 5, 2014.
16. Murray, M.D., Morrow, D.G., Weiner, M., Clark, D.O., Tu, W., Deer, M.M., Brater, C, Weinberger, M. (2004). A conceptual framework to study medication adherence in older adults. American Journal of Geriatric Pharmacology, 2(1):36-41.
17. Woodruff K. (2010). Preventing Polypharmacy in Older Adults. American Nurse Today 5(10). Available online at:https://www.medscape.com/viewarticle/732131_1. Last accessed Sept. 5, 2014.
18. Schafer, S.L. (2001). Prescribing for seniors: It’s a balancing act. Journal of the American Academy of Nurse Practitioners, 13(3):108-112.
19. Jeff E. Freund J.E., Martin B.A., Kieser M.A., Williams S.M., Sutter S.L. (2013). Transitions in Care: Medication Reconciliation in the Community Pharmacy Setting After Discharge. Innovations in Pharmacy, 4(2). Available online at:https://www.pharmacy.umn.edu/innovations/prod/groups/cop/%40pub/%40cop/%40innov/documents/article/cop_article_438952.pdf. Last accessed Sept. 5, 2014.
20. Quality Insights Pennsylvania (2014). Transitions in Care and Medication Reconciliation in the Older Adult Population. Content prepared by VHQC. Available online at: http://www.qipa.org/getattachment/6f04681a-cea2-4f63-8e0c-f0c145423bfd/Transitions-in-Care-and-Med-Reconciliation-PA_508.aspx. Last accessed May 14, 2015.
21. Institute for Healthcare Improvement. Available online at:http://www.ihi.org/resources/Pages/Changes/ReconcileMedicationsatAllTransitionPoints.aspx. Last accessed Sept. 5, 2014.
22. Kripalani, S., Jackson, A.T., Schnipper, J.L., Coleman, E.A. (2007). Promoting effective transitions of care at hospital discharge: A review of key issues for hospitalists. Journal of Hospital Medicine, 2(5):314-323.
23. Osterberg, L., Balschke, T. (2005). Adherence to Medication. The New England Journal of Medicine, 353(5):487-497.
24. Gurwitz, J.H., Field, T.S., Harrold, L.R., Rothschild, F., Debellis, K., Seger, A.C., Cadoret, C., Fish, L.S., Garber, L., Kelleher, M., Bates, D.W. (2003). Incidence and preventability of adverse drug events among older persons in the ambulatory setting. Journal of the American Medical Association, 289(9):1107-1116.
25. Marek, K.D., Lisa Antle, L. (2009). Medication Management of the Community-Dwelling Older Adult. Available online at:https://www.ncbi.nlm.nih.gov/books/NBK2670/. Last accessed Sept. 5, 2014.
26. Gellad, W.F., Grenard, J., McGlynn, E.A. (2009). A review of barriers to medication adherence: A framework for driving policy options. Available online at: https://www.rand.org/content/dam/rand/pubs/technical_reports/2009/RAND_TR765.pdf. Last accessed July 14, 2014.
27. National Council on Patient Information and Education (2007). Enhancing prescription medication adherence: A national action plan. Available online at: https://bemedwise.org/docs/enhancingprescriptionmedicineadherence.pdf. Last accessed July 14, 2014.
28. Conn, V.S., Hafdahl, A.R., Cooper, P.S., Ruppar, T.M., Mehr, D.R., Russell, C.L. (2009). Interventions to improve medication adherence among older adults: Meta-analysis of adherence outcomes among randomized controlled trials. The Gerontologist, 49(4):447-462.
29. Unite for Sight. Issues in Medication Management. Available online at: http://www.uniteforsight.org/global-health-university/medication-adherence. Last accessed Sept. 8, 2014.
30. Jencks, S.F., Williams, M.V., Coleman, E.A. (2009). Rehospitalizations among patients in the Medicare fee-for-service program. New Engl J Med, 360(14):1418-1428.
31. Osterberg, L., Blaschke, T. (2005). Adherence to medication. N Engl J Med, 353(5): 487-497.
32. Consult Pharm. 2007 Apr; 22(4):355-61. Guidelines for medication therapy management services in long-term care facilities. Available online at: https://www.ascp.com/sites/default/files/ASCP-PA-NewcomentsGuidelines07MTM.pdf. Last accessed August 5, 2014.
33. ASCP Guidelines for Medication Therapy Management Services in Long-Term Care Facilities. Available online at:http://www.ascp.com/resources/policy/upload/ASCP-MTMGuidelines-3-3-07-3.pdf. Last accessed Sept. 1, 2014.
34. American Society of Consultant Pharmacists. Available online at: https://www.ascp.com/articles/beers-list-criteria. Last accessed Sept. 5, 2014.
35. Gallagher, P., Ryan, C., Byrne, S., Kennedy, J., O’Mahony, D. (2008). STOPP (Screening Tool of Older Persons’ Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther., 46(2):72-83. Available online at: https://www.ncbi.nlm.nih.gov/pubmed/18218287. Last accessed Sept. 8, 2014.
36. RazaHaque, M.D. (2009). ARMOR: A Tool to Evaluate Polypharmacy in Elderly Persons. Annals of Long-Term Care, 17(6). Available online at: https://www.managedhealthcareconnect.com/content/armor-a-tool-evaluate-polypharmacy-elderly-persons. Last accessed Sept. 5, 2014.
37. Zermansky, A.G., Petty, D.R, Raynor, D.K., Freemantle, N., Vail, A., Lowe, C.J (2001). Randomized controlled trial of clinical medication review by a pharmacist of elderly patients receiving repeat prescriptions in general practice. BMJ, 3:1340-1343.
38. Furness, L., Burns, A., Craig, S., Scobie, S., Cooke, J., Faracher, B. (2000). Effects of a pharmacist’s medication review in nursing homes: randomized controlled trail. The British Journal of Psychiatry, 563-577.
39. Pham, C.B., Dickman, R.L. (2007). Minimizing Adverse Drug Events in Older Patients. AmFam Physician, 76(12):1837-1844. Available online at: https://www.aafp.org/afp/2007/1215/p1837.html. Last accessed July 11, 2014.
40. Reducing and Preventing Adverse Drug Events to Reduce Hospital Costs, Research in Action, Issue 1. March 2001 Agency for Healthcare Research and Quality, Rockville, MD. Available online at: http://www.ahrq.gov/research/findings/factsheets/errors-safety/aderia/index.html. Last accessed Sept. 8, 2014.
41. Medication Therapy Management in Pharmacy Practice. Core Elements of an MTM Service Model. Version 2.0. American Pharmacists Association and National Association of Chain Drug Stores Foundation. March 2008. Available online at:https://www.accp.com/docs/positions/misc/CoreElements.pdf.
42. Bunting, B.A., Smith, B.H., Sutherland, S.E. (2008). The Asheville Project: clinical and economic outcomes of a community-based long-term medication therapy management program for hypertension and dyslipidemia. Journal of the American Pharmacists Association (JAPhA), 48(1):23-31.
43. Planas, L.G., Crosby, K.M., Mitchell, K.D., Farmer, K.C. (2009). Evaluation of a hypertension medication therapy management program in patients with diabetes. Journal of the American Pharmacists Association (JAPhA), 49(2):164-170.
44. Medicare Prescription Drug, Improvement, and Modernization Act of 2003, Public Law 108-173. Available online at:http://www.gpo.gov/fdsys/pkg/PLAW-108publ173/content-detail.html. Last accessed Sept. 8, 2014.
45. Medication Therapy Management in Chronically Ill Populations: Final Report. August 2013. Acumen. Available online at:https://innovation.cms.gov/Files/reports/MTM_Final_Report.pdf. Last accessed Sept. 1, 2014.
46. Medication Therapy Management in Chronically Ill Populations: Final Report. August 2013. Acumen. Available online at:https://innovation.cms.gov/Files/reports/MTM_Final_Report.pdf. Last accessed Sept. 1, 2014.
47. American Society of Consultant Pharmacists. Available online at: https://www.ascp.com/articles/beers-list-criteria. Last accessed Sept. 8, 2014.
48. Gallagher, P., Ryan, C., Byrne, S., Kennedy, J., O’Mahony, D. (2008). STOPP (Screening Tool of Older Persons’ Prescriptions) and START (Screening Tool to Alert doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther., 46(2):72-83. Available online at: https://www.ncbi.nlm.nih.gov/pubmed/18218287. Last accessed Sept. 8, 2014.
49. RazaHaque, M.D. (2009). ARMOR: A Tool to Evaluate Polypharmacy in Elderly Persons. Annals of Long-Term Care, 17(6). Available online at: https://www.managedhealthcareconnect.com/content/armor-a-tool-evaluate-polypharmacy-elderly-persons. Last accessed Sept. 5, 2014.
50. Quality Insights Pennsylvania (2014). Transitions in Care and Medication Reconciliation in the Older Adult Population. Content prepared by VHQC. Available online at: http://www.qipa.org/getattachment/6f04681a-cea2-4f63-8e0c-f0c145423bfd/Transitions-in-Care-and-Med-Reconciliation-PA_508.aspx. Last accessed May 14, 2015.
51. Institute for Healthcare Improvement. Available online at:http://www.ihi.org/topics/ADEsMedicationReconciliation/Pages/default.aspx. Last accessed Sept. 8, 2014.
52. MATCH Medication Reconciliation Toolkit. Available online at: https://www.ahrq.gov/sites/default/files/wysiwyg/professionals/quality-patient-safety/patient-safety-resources/resources/match/match.pdf. Last accessed Sept. 8, 2014.
53. Agency for Healthcare Research and Quality (2008). Patient Safety and Quality: An Evidence-Based Handbook for Nurses (2008). Publication No. 08-0043.
54. Cline, C.M., Bjorck-Linne, A.K., Israelsson B.Y., et al. (1999). Non-compliance and knowledge of prescribed medication in elderly patients with heart failure. Eur J Heart Fail, 1(2):145–9.
55. Pinto Pereira, L.M., Clement, Y., Da Silva, C.K., et al. (2002) Understanding and use of inhaler medication by asthmatics in specialty care in Trinidad: a study following development of Caribbean guidelines for asthma management and prevention. Chest, 121(6):1833–40.
56. Barat, I., Andreasen, F., Damsgaard, E.M. (2001). Drug therapy in the elderly: what doctors believe and patients actually do. Br J Clin Pharmacol, 51(6):615–22.
57. Morrell, R.W., Park, D.C., Poon, L.W. (1990). Effects of labeling techniques on memory and comprehension of prescription information in young and old adults. J Gerontol, 45(4):P166–72.
58. Cargill, J.M. (1992). Medication compliance in elderly people: influencing variables and interventions. J Adv Nurs, 17(4):422–6.
59. Bodenheimer, T., Lorig, K., Holman, H., Grumbach, K. (2002). Patient self-management of chronic disease in primary care. JAMA 288:2469-2475.
60. Lorig, K.R., Sobel, D.S., Ritter, P.L., Laurent, D., Hobbs, M. (2001). Effect of a self-management program on patients with chronic disease. Eff Clin Pract, 4:256-262.
61. Bodenheimer, T., Lorig, K., Holman, H., Grumbach, K. (2002). Patient self-management of chronic disease in primary care. JAMA, 288:2469-2475.
62. Electronic health record. Available online at: https://www.himss.org/library/ehr/%3FnavItemNumber%3D13261. Last accessed June 17, 2014.
63. Enabling medication management through health IT: Review protocol. Rockville, MD: U.S. Department of Health and Human Services. Available online at: https://www.ahrq.gov/prevention/guidelines/index.html. Last accessed June 17, 2014.
64. ONC Safer Guide: Computerized Order Entry with Decision Support. Available online at:https://www.healthit.gov/safer/guide/sg007. Last accessed July 07, 2014.
65. Meredith, S., Feldman, P.H., Frey, D., Hall, K., Arnold, K., Brown, N.J., Ray, W.A. (2001). Possible medication errors in home healthcare patients. Journal of the American Geriatric Society, 49(6):719-724.
66. Health IT Standards and EHR Requirements and Activities for LTPAC. Available online at:http://www.ltpachealthit.org/sites/default/files/Health_IT_Standards_and_EHR_Requirements_and_Activities_for_LTPACFlyer%20Format(5).pdf. Last accessed Sept. 1, 2014
67. Preparing for Medicare Part D Requirements for e-Prescribing on Long-Term Care. Available online at:http://www.ncpdp.org/NCPDP/media/pdf/NCPDPePrescribinginLTCMedicareDWebinar.pdf. Last accessed Sept. 1, 2014.
68. ePrescribing of Controlled Substances (EPCS): Overview, State Readiness and Certified Vendors:http://surescripts.com/products-and-services/e-prescribing-of-controlled-substances. Last accessed Apr. 13, 2015.
69. Preparing for Medicare Part D Requirements for e-Prescribing on Long-Term Care. Available online at:http://www.ncpdp.org/NCPDP/media/pdf/NCPDPePrescribinginLTCMedicareDWebinar.pdf. Last accessed Sept. 1, 2014.
70. Enabling medication management through health IT: Review protocol. Rockville, MD: U.S. Department of Health and Human Services. Available online at: https://www.ahrq.gov/prevention/guidelines/index.html. Last accessed June 17, 2014.
71. Kimber, M.B., Peterson, G.M. (2006). Telepharmacy — Enabling technology to provide quality pharmacy services in rural and remote communities. Journal of Pharmacy and Research, 36(2), 128-133.
72. Sherman, J. (2007). Telepharmacy – A promising alternative for rural communities. Pharmacy Times, 73(2):65-86.
73. Peterson, C.D., Anderson, H.C. (2002). Chapter 10: Telepharmacy. Available online at:https://www.ndsu.edu/fileadmin/telepharmacy/TELEPHARMACY-TAD1.pdf. Last accessed July 7, 2014.
74. Hillestad, R., Bigelow, J., Bower, A., Girosi, F., Meili, R., Scoville, R., Taylor, R. (2005). Can electronic medical record systems transform health care? Potential health benefits, savings, and costs. Health Affairs, 24(5):1103-1117.
75. Center for Technology and Aging (2009). Technologies for optimizing medication use in older adults. Available online at:http://www.techandaging.org/MedOpPositionPaper.pdf. Last accessed July 7, 2014.
76. Fuson, S. (2010). Choosing a medication reminder system. Today’s Caregiver. Available online at:https://caregiver.com/channels/medication/articles/medication_reminder_system.htm. Last accessed July 7, 2014.
77. Wakefield, B.J., Orris, L.J., Holman, R.E., Russell, C.L. (2008). User perceptions of in-home medication dispensing devices. Journal of Gerontological Nursing, 34(7):15-24.
78. Law, T., Ma, B., Icuss, J., Klopfer, M. (2008). In-Home Automated Medication Management and Dispensing System. 2007-2008 RERC-AMI Student Design Competition, University of California, Irvine, Henry Samueli School of Engineering.
79. Wakefield, B.J., Orris, L.J., Holman, R.E., Russell, C.L. (2008). User perceptions of in-home medication dispensing devices. Journal of Gerontological Nursing, 34(7):15-24.
80. Center for Improving Medication Management, eHealth Initiative (2008). Electronic prescribing: Becoming mainstream practice. Available online at: http://www.thecimm.org/PDF/eHI_CIMM_ePrescribing_Report_6-10-08.pdf. Last accessed July 7, 2014.
81. Bell, D.S., Friedman, M.A. (2005). E-prescribing and the Medicare Modernization Act of 2003. Health Affairs, 24(5):1159-1169.
82. Kawamoto, K., Houlihan, C.A., Balas, E.A., Lobach, D.F. (2005). Improving clinical practice using clinical decision support systems: A systematic review of trials to identify features critical to success. British Medical Journal, 330(7494), 765.
83. Ammenwerth, E., Schnell-Inderst, P., Machan, C., Siebert, U. (2008). The effect of electronic prescribing on medication errors and adverse drug events: A systematic review. Journal of American Medical Informatics Association, 15(5):585-600. Available online at: https://academic.oup.com/jamia. Last accessed Sept. 8, 2014.
84. Radley, D.C., Wasserman, M.R., Olsho, L.E.W., Shoemaker, S.J., Spranca, M.D., Bradshaw, B. (2013). Reduction in medication errors in hospitals due to adoption of computerized provider order entry systems. Journal of the American Medical Informatics Association, 20:470-476. Available online at: https://academic.oup.com/jamia. Last accessed July 07, 2014.
85. Simon, S.R., Smith, D.H., Feldstein, A.C., Perrin, N., Yang, X., Zhou, Y., Platt, R., Soumerai, S.B. (2006). Computerized prescribing alerts and group academic detailing to reduce the use of potentially inappropriate medications in older people. Journal of the American Geriatrics Society, 54(6):963-968.
86. First Consulting Group, “Computerized Physician Order Entry: Costs, Benefits, and Challenges — A Case Study Approach.” Report prepared for the Massachusetts Technology Collaborative & New England Healthcare Institute, Fall 2004.
87. Handler, S.M., Hanlon, J.T., Perera, S., Saul, M.I., Fridsma, D.B., Visweswaran, S., Studenski, S.A., Roumani, Y.F., Castle, N.G., Nace, D.A., Becich, M.J. (2008). Assessing the performance characteristics of signals used by a clinical event monitor to detect adverse drug reactions in the nursing home. American Medical Informatic Association Annual Symposium Proceedings Archive, 6:278-282.
88. Field, T.S., Rochon, P., Lee, M., Gavendo, L., Baril, J.L., Gurwitz, J.H. (2009). Computerized clinical decision support during medication ordering for long-term care residents with renal insufficiency. Journal of the American Medical Informatics Association, 16(4):480-485.
89. Subramanian, S., et al. (2012). Immediate financial impact of computerized clinical decision support for long-term care residents with renal insufficiency: a case study. Journal of the American Medical Informatics Association, 19(3):439-42.
90. Casey, M.M., Sorensen, T.D., Elias, W., Knudson, A., and Gregg, W. (2010). Current practice and state regulations regarding telepharmacy in rural hospitals. American Journal of Health-System Pharmacy 69(8):1085-1092.
91. Oren, E., Shaffer, E.R., Guglielmo, B.J. (2003). Impact of emerging technologies on medication errors and adverse drug events. American Journal of Health-System Pharmacy, 60(14):1447-1457.
92. National Academy of Sciences (2007). Preventing medication errors: Quality chasm series. Available online at:https://www.nap.edu/catalog/11623/preventing-medication-errors. Last accessed April 3, 2014.
93. Poon, E.G., Keohane, C.A., Yoon, C.S., Ditmore, Mm, Bane, Am, Levtzion-Korach, Om, Moniz, Tm, Rothschild, J.M., Kachalia, A.B, Hayes, J., Churchill, W.W., Lipsitz, S., Whittemore, A.D., Bates, D.W., Gandhi, T.K. (2010). Effect of bar-code technology on the safety of medication administration. The New England Journal of Medicine, 362(18):1698-1707.
94. Clinical Update (2009). Strategies to reduce medication errors in older adults. Australian Nursing Journal, 17(3):30-33.
95. Center for Connected Health (2010). Wireless medication adherence: Reminders and incentives improve adherence. Available online at: http://www.connectedhealth.org/media/288561/vitality 20interim%20data%20release%206.23.10.pdf. Last accessed July 7, 2014.
96. Winland-Brown, J.E., Valiente, J. (2000). Effectiveness of different medication management approaches for elders’ medication adherence. Outcomes Management for Nursing Practice, 4(4):172-176.
97. Buckwalter, K.C., Wakefield, B.T., Hanna, B., Lehman, J. (2004). New technology for medication adherence: Electronically managed medication dispensing system. Journal of Gerontological Nursing, 30(7):5-8.
98. Kaushal, R., Jha, A.K., Franz, C., Glaser, B., Kuperman, G.J., Khorasani, R., Tanasijevic, M., Bates, D.W. (2006). Return on investment for computerized physician order entry systems. Journal of the American Medical Informatics Association, 13(3):261-266.
99. Maviglia, S.M. ,Yoo, J.Y, Franz, C., Featherstone, E., Churchill, W., Bates, D.W., Gandhi, T.K., Poon, E.G. (2007). Cost-benefit analysis of a hospital pharmacy bar code solution. Archives of Internal Medicine, 167(8):788-794.
100. Medicaid Waivers Information, Medicaid. Available online at: https://www.medicaid.gov/medicaid/section-1115-demo/index.html. Last accessed June 22, 2013.
101. CAST Analysis of State Payment for Aging Services Technologies. Available online at: https://www.leadingage.org/sites/default/files/CAST_State_Paymen_%20Analysis.pdf? . Last accessed Sept. 8, 2014.
102. The Importance of Home and Community Based Settings in Population Health Management, Philips Whitepaper, March 2013. Available online at: https://www.leadingage.org/sites/default/files/The_importance_of_home_and_community_March_2013_1.pdf. Last accessed Sept. 8, 2014.
103. CMMI Innovations Models and Initiatives, CMMI, CMS. Available online at:https://innovation.cms.gov/initiatives/index.html. Last accessed June 22, 2013.
104. Technology Related Provisions in the ACA, LeadingAge CAST. Available online at:https://leadingage.org/resources/affordable-care-act-technology-provisions Last accessed June 22, 2013.
Medicare Hospital Readmission Reduction Program, CMS. Available online at: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Last accessed June 22, 2013.
106. CMS ACO Initiatives, CMMI, CMS. Available online at: https://innovation.cms.gov/initiatives/ACO/. Last accessed June 22, 2013.
107. Retrospective Acute Hospital Stay plus Post-Acute Services Payment Bundling Demonstration, CMMI, CMS. Available online at: https://innovation.cms.gov/initiatives/BPCI-Model-2/. Last accessed June 22, 2013.
108. Retrospective Post-Acute Care Only Payment Bundling Demonstration, CMMI, CMS. Available online at:https://innovation.cms.gov/initiatives/BPCI-Model-3/. Last accessed June 22, 2013.
109. Innovations in Medication Therapy Management: Effective Practices for Diabetes Care and Other Chronic Conditions. Available online at: https://www.ahip.org/Innovations-in-Medication-Therapy-Management/. Last Accessed Sept. 1, 2014.
110. Ellenbecker, C.H., Samia, L.,Cushman, M.J., Alster, K. Patient Safety and Quality in Home Health Care Available online at: https://www.ncbi.nlm.nih.gov/books/NBK2631/. Last accessed Sept. 5, 2014.
111. Ellenbecker, C.H., Samia, L.,Cushman, M.J., Alster, K. Patient Safety and Quality in Home Health Care Available online at: http://www.ncbi.nlm.nih.gov/books/NBK2631/. Last accessed Sept. 5, 2014.
112. Environmental Scan of Instruments to Inform Consumer Choice in Assisted Living Facilities, Assisted Living Defined. Available online at: https://innovations.ahrq.gov/qualitytools/environmental-scan-instruments-inform-consumer-choice-assisted-living-facilities. Last accessed May 14, 2014.
113. Environmental Scan of Instruments to Inform Consumer Choice in Assisted Living Facilities, Assisted Living Defined. Available online at: https://innovations.ahrq.gov/qualitytools/environmental-scan-instruments-inform-consumer-choice-assisted-living-facilities. Last accessed May 14, 2014.
114. Alwan M. (2013). Alma’s Technology: A Look at Medication Adherence Technologies. Available online at:http://www.leadingage.org/cast/resources/high-tech-aging-improving-lives-today. Last accessed Sept. 2, 2014.