
Shared Care Planning and Coordination for Long-Term and Post-Acute Care: A Primer and Provider Selection Guide
1 Purpose of White Paper and Executive Summary
1.1 Purpose of White Paper
1.2 Executive Summary
1.3 Disclaimer
2 Shared Care Planning and Coordination
2.1 Definition
2.2 Perspectives on Care Planning and Coordination
2.2.1 Patient and Family Perspective
2.2.2 Care Professionals Perspective
2.2.3 Payer’s Perspective
2.2.4 System Representatives Perspective
2.3 Care Coordination and Disease Management Programs
2.4 Care Planning and Coordination Models
2.4.1 Social Models
2.4.2 Medically Oriented Models
2.4.3 Integrated Models
3 Types of Care Planning and Coordination Technologies (non-mutually exclusive categories)
3.1 Care Planning and Coordination Tools
3.1.1 Shared Care Planning Tools
3.1.2 Care Management and Case Management Tools
3.1.3 Care Coordination and Communications Portals/Tools
3.2 Sources of Information
3.3 Enabling Technologies
3.3.1 Interoperability
3.3.2 Health Information Exchange
3.3.3 Information Repositories
3.3.4 APIs
4 Potential Uses of Care Planning and Coordination Technologies
5 Potential Benefits of Care Coordination and Care Planning Technologies
5.1 Improved Health Outcomes
5.2 Hospitalizations, Hospital Length of Stay, and Emergency Department Visits
5.3 Prolonging Independence and Reducing Long-Term Care Costs
6 Potential LTPAC Provider Business Models
6.1 Medicare Coverage
6.1.1 Care Plan Oversight
6.1.2 Chronic Care Management
6.1.3 Transitional Care Management
6.2 Medicaid Coverage
6.3 Program of All-Inclusive Care for the Elderly (PACE)
6.4 Private Health Insurance Coverage
6.5 Potential Affordable Care Act (ACA) Opportunities
6.6 Private Pay
6.7 Standard of Care and Other Payment Sources
6.8 Return on Investment (ROI) of Care Planning and Coordination
6.8.1 ROI to Patients and/or their Families
6.8.2 ROI to Payers
6.8.3 ROI to Care Provider
6.8.4 Online ROI Calculator
7 Planning for and Selecting Appropriate Care Planning and Coordination Technology
7.1 Understanding the Population, Issues, Care Settings, Needed Services, and Care Partners
7.2 Planning for Care Planning and Coordination Solutions
7.2.1 Visioning and Strategic Planning
7.2.2 Organizational Readiness Assessment
7.2.3 Operational Planning
8 Care Planning and Coordination Matrix Components
9 Acknowledgement of Contributors
9.1 Contributing Writers
9.2 Workgroup Members
9.3 Participating Care Planning and Coordination Vendors
10 References and Resources
1. Purpose of White Paper and Executive Summary
1.1 Purpose of White Paper
The purpose of this paper is to aid LeadingAge and other aging services organizations in understanding the range of shared care planning and coordination technologies available in the marketplace, their uses, and their benefits. In addition, the white paper will help providers plan for, select, and implement such solutions. The paper will also include a matrix of existing shared care planning and coordination solutions that will help providers select solutions that best fit their requirements.
1.2 Executive Summary
Care planning and coordination involves creating a care plan, a personalized written statement of a care recipient’s comprehensive health and social support assessed needs. It sets out what support providers and caregivers should deliver, why and when, and who is meant to provide it.
The ability to communicate with, and educate, patients at home is an important feature for care management. Technology that accomplishes these goals can provide substantial benefits. Care planning and coordination technologies can educate patients and help them manage chronic diseases, support and stabilize post-acute patients, ease shared care and care transitions, and coordinate support services for older adults. The purpose of this paper is to aid LeadingAge members and other aging services organizations in understanding the range of shared care planning and coordination technologies available in the marketplace, their uses, and their benefits.
Research shows that care coordination and care planning technologies have the potential to improve health and reduce hospitalizations, length of hospital stays, emergency department visits, and laboratory tests. For example, one non-randomized but controlled study of Linkcare®, which supports advanced case management with shared-care plans across health care tiers and offers integration with provider-specific electronic health records, found that Linkcare® produced success in four areas:
- It facilitated long-term sustainability of training effects in rehabilitation and active life style,
- It showed significant positive outcomes in enhanced care,
- It reduced on average five in-hospital days per patient with a 30-day re-admission rate of 10%; and
- It enhanced community-based quality forced spirometry testing.
In an aging in place community, sensors that alerted care coordinators to changes in health status have enabled older adults to stay in the community longer, giving them independence and saving them potential nursing home costs of $30,000 per person. These initial results are impressive.
Forward-thinking senior living providers can be at the forefront of this trend. They can provide virtual support at home by leveraging interactive connected care platforms and their skill sets—and lead the way in forming new, innovative care delivery models.
This white paper can assist you in selecting the best technology for your organization. We take you through the process of understanding shared care planning and coordination, including how it helps diverse parties from the patient and family caregivers to providers, payers, and the system. We discuss the different care planning and coordination models and available technology tools as well as discuss enabling technologies.
The paper explains available provider business models that would encourage care planning coordination, and consequently the adoption of related technologies. These include the Program of All-Inclusive Care for the Elderly (PACE) and opportunities brought by the Affordable Care Act (ACA). Other potential opportunities may exist under Medicare, Medicaid, private health insurance, private pay, and services offered by long-term post-acute care and other providers as standard of care.
To get you quickly to the information you need, each main section also includes a brief overview of the section’s contents. The white paper concludes with a review of the CAST Shared Care Planning and Coordination Selection Matrix and Online Selection Tool that can help you thoroughly evaluate available technologies and select the best solution for your organization.
1.3 Disclaimer
This information is meant to assist in understanding Shared Care Planning and Coordination technologies, but it cannot possibly include all systems that may be available. Products mentioned in this report are only illustrative examples and have not been tested, independently evaluated, or endorsed by LeadingAge or LeadingAge CAST. Please use this paper as a general guideline in understanding functionalities and examples of current Shared Care Planning and Coordination systems. Where appropriate, provider case studies were identified.
2. Shared Care Planning and Coordination
2.1 Definition
What Care Plans Do
Care plans do the following:
- Provide caregivers with detailed guidance;
- Encourage documentation of care;
- Facilitate continuity of care between different staff members and across shifts; and
- Support care coordination, especially during transitions of care.
A comprehensive shared care plan can be put together by a multi-disciplinary team from different provider organizations that deliver care and support, with input from the patient and family.1 It should allow a clinician or caregiver to view information that is directly relevant to his or her role in caring for the patient, to easily identify who is doing what, and to update other members of an interdisciplinary team on new developments.
- It should put the patient’s goals (captured in his or her own words) at the center of decision-making and give that person direct access to his or her information.
- It should be holistic and describe both clinical and nonclinical (including home- and community-based) needs and services.
- It should follow the person through high-need episodes (e.g., acute illness), as well as periods of health improvement and maintenance.
Care coordination means coordinating the work of two or more caregivers to carry out the care plan.
Care coordination means coordinating the work of two or more caregivers to carry out the care plan. It involves deliberately organizing processes created by different entities, such as an organization, health care entity or a care team from different organizations. Care coordination also supports shared care, where multiple caregivers or care providers deliver care to the individual in the same place and/or deliver the same level of care, or are working to transition the patient seamlessly from one setting or level of care to another.
The main goal of care coordination is to share information to meet the patient’s needs in a safe and effective manner and to deliver optimal quality of care.
Why Does Care Coordination Matter?
Care coordination is identified by the Institute of Medicine as a key strategy that has the potential to improve the effectiveness, safety, and efficiency of the American health care system. Well-designed, targeted care coordination that is delivered by the right people can improve outcomes for everyone: patients, providers, and payers.2
The 21st century has brought new challenges, including technology advancements, that have created an interconnected and fast-moving world. In many ways, technology has improved communication across the health care continuum; however, it is not a flawless system.3 The infrastructure of technology is so varied and intricate that communication between some systems is splintered even within the same organization, let alone between a hospital and a nursing home or home and community-based provider.
Technology, when well-designed and thoroughly integrated, can support care planning and coordination, resulting in improved outcomes for all stakeholders engaged in care, including individuals receiving care, providers, and payers.4
2.2 Perspectives on Care Planning and Coordination
2.2.1 Patient and Family Perspective
In a 2008 paper, Thomas Bodenheimer observed that care coordination is often perceived only as interactions among different care providers (provider-provider coordination). However, he concluded that care coordination should also include interactions among providers, patients, and families (provider-family coordination). Considering these points, we can assume that good communication among all parties involved in the patient’s health care is an essential part of providing excellent care.5
When a loved one is suffering from complex medical conditions that require interventions and follow up from multiple medical specialists and family members, managing multiple details can easily overwhelm and confuse patients.
For a family member caregiver, care coordination is vital for a successful care transition without the often-seen increase in caregiver anxiety. For example, Collins and Swartz discuss how placing a care recipient into a long-term care facility is not associated with positive effects and may increase caregiver anxiety.6 Based on this, it is reasonable to assume that any transition of care, whether from a hospital to a nursing home, a hospital to the community, or for that matter any other transition, will increase caregiver anxiety, potentially leading to family tension.
Patients and their caregivers must be given the chance to help define the care plan.
Keys to Success
To have an optimal care transition, it is vital to have good communication among patients and all parties involved in caring for them.
Patients with complex care needs, and their caregivers, must be informed of what to expect before, during, and after a transition. They must also be given the opportunity to help define the care plan so that their values and preferences are honored and reflected in it.7
2.2.2 Care Professionals Perspective
Numerous professionals work together to coordinate patient care. This group may include nurses, nurse practitioners, social workers, physicians, physician assistants, therapists, insurance representatives, contractual service vendors, and others.
Any of these professionals may function as the case manager and lead the charge for a patient’s care coordination. However, in reality this process usually becomes fragmented among the variety of providers involved. Communication of patient needs, prioritization, and scheduling of services requires extensive time, usually with no reimbursement. Basic care coordination involves assessing and identifying patient needs, developing a plan of care, implementing the plan, and evaluating the outcomes observed. For patients suffering with extensive chronic conditions and/or multiple comorbidities, care coordination takes on a life of its own, requiring a conglomerate of service providers.
Patients and their caregivers must be given the chance to help define the care plan.
The care professional’s perspective on care planning and coordination may vary depending on their role in health care delivery. Practitioners may be reluctant to use these programs because they limit autonomy and may reduce pay for services.8 According to Zweifel, a study indicated care professionals were reluctant to participate in care management activities that would impact income and shared decision making.9
The Centers for Medicare & Medicaid Services (CMS) reported that about 35 million Medicare beneficiaries are eligible to receive billable care-management services. But the agency has received reimbursement requests for only about 100,000. Complaints about chronic care management reimbursed programs vary from lengthy documentation to having to have a difficult conversation with patients who now are responsible for a 20% copayment for previously free service.10 These factors suggest that professionals see care planning and coordination as time consuming, and have less desire to participate.
With the recent shift from pay for service to pay for performance and the emphasis on person-centered care in United States health care, the role of care coordinator or case manager is becoming accepted. In some practices, this person now facilitates care coordination.
Several factors may quell professionals’ fears of care coordination’s impact on revenue, practice independence, and control of services: the building of health care networks, bundling of services, and implementation of care management over time. Numerous companies now provide successful and cost-effective care management services. For example, WellMed uses data to stratify patients based on their risk stratification to maximize services for the neediest patients while ensuring the right structure of care in the right environment for the less needy patients. The result is a cost-effective quality care model. Efforts to share this model and gain support with care planning professionals is ongoing.
Chronic Care Management (CCM), and the ability of a care provider to bill for CCM or contract the CCM service to another party, may influence how today’s health care planner or care coordinator feel about care planning. Due to the growth of care management as a billable service, care professionals’ participation and opinions on care planning and coordination will continue to evolve.
2.2.3 Payer’s Perspective
Medicare, the federal health insurance program, is the primary payer for 55 million people ages 65 and over and for people with total disabilities. Medicare helps to pay for hospital and physician visits, prescription drugs, and other acute and post-acute services. In 2014, spending on Medicare accounted for 14% of the federal budget.11
Traditionally, Medicare pays providers for individual services, which can fragment care.
Medicare plays a major role in the health care system, accounting for 22% of total national health spending. In 2013, 26% of spending was for hospital care and 22% for physician services, according to a Congressional Budget Office report in March 2015.
Traditionally, Medicare makes separate payments to providers for the individual services they furnish to beneficiaries for a single illness or course of treatment. This approach can result in fragmented care with minimal coordination across providers and health care settings. Payment rewards the quantity of services offered by providers rather than the quality of care furnished. Research has shown that bundled payments can align incentives for providers, hospitals, post-acute care providers, physicians, and other practitioners, allowing them to work closely together across all specialties and settings.12
The Bundled Payments for Care Improvement Initiative (BPCI) was developed by the Center for Medicare & Medicaid Innovation (Innovation Center). The Affordable Care Act created the Innovation Center to test innovative payment and service delivery models that have the potential to reduce Medicare, Medicaid, and Children’s Health Insurance Program (CHIP) expenditures, while preserving or enhancing the quality of care for beneficiaries. Bundled payment is defined as the reimbursement of health care providers (such as hospitals and physicians) “on the basis of expected costs for clinically defined episodes of care.” This model will required care coordination among all providers.13
The Centers for Medicare & Medicaid Services (CMS) is committed to ensuring that beneficiaries receiving care from providers participating in BPCI receive high-quality care. To that end, CMS is actively monitoring the quality of beneficiaries’ care. CMS is analyzing quality information available from claims and quality reporting from the awardees, as well as surveys and patient assessment tools to assess care experience and health outcomes.
The CMS monitoring effort aims to identify quality improvements, including process improvements, changes in outcomes, and lower costs. It is also designed to detect inappropriate practices including care stinting, patient selection to maximize financial gain, and cost shifting. Participants must comply with and participate in Evaluation and Monitoring activities and data collection efforts. Providers who fail to deliver optimal outcomes will pay penalties.
BPCI is only one such program that CMS is using to tie payments to outcome, and away from service, where shared care planning and coordination can play a significant role in reducing cost and improving care. Private payers are also experimenting with their own innovative models.
One broad approach for achieving care coordination is to include health information technologies such as electronic health records (EHR). Interoperable EHR systems can improve care planning and coordination and decrease fragmented care. They have the potential to integrate and organize patient health information, and to instantly distribute it among all authorized providers involved in a patient’s care.
2.2.4 System Representatives Perspective
With health information technology (IT) and electronic health records (EHRs), every provider can have accurate and up-to-date information about a patient. This is especially important with patients who are making transitions between care settings. Better care coordination can lead to better quality of care and improved patient outcomes.
Health IT and EHRs can give every provider up-to-date information about a patient.
Leveraging health IT across the continuum of care allows for the following:
- Improved information sharing and better integration among providers;
- Up-to-date medication and allergy lists;
- Order entry at point of care or off-site;
- Standardization of data, order sets, and care plans helping to implement common treatment of patients using evidence-based medicine;
- Access to experts for rural health care providers, by sharing best practices and allowing for specialized care through telemedicine;
- Population management trended data and treatment and outcome studies;
- More convenient, faster, and simpler disease management; and
- Communication with others on the care team.
EHRs must give the end user a way to synthesize data into useful information and knowledge to help ensure the patient receives the best care plan and coordination. Users such as physicians and nurses must know and understand the care plan based on the patient’s needs, and the case management and coordination of care the patient needs based on his or her conditions and circumstances.
System representatives view the health IT and the EHR only as tools. Organizations purchasing and implementing these tools must decide how to use them. Systems that have features like interoperability with other systems and health information exchange capabilities, including the seamless connection to care planning and coordination modules, can create enhanced efficiency in health care coordination and delivery. Attaining this efficiency, however, depends completely on the end-user training and ability to use the system’s capabilities.
Care planning modules in an EHR should be designed to guide users to describe and document interventions based on the patient’s background information, assessments, and goals, and to monitor the outcomes.
Care coordination, in contrast, should track a patient from the physician’s office to the hospital or nursing home. It should include needs, observations, results, and consultation notes in an effort to ensure services are not duplicated and do not interact with each other. These systems must be able to interface and exchange information with a number of information systems, such as other EHRs, patient portals, health information exchange entities, etc., to keep the care plan up-to-date and to maximize timeliness, efficacy, and effectiveness of care coordination.
2.3 Care Coordination and Disease Management Programs
Health care is continuously evolving. As new drugs, diagnostic procedures, treatments, and interventions are introduced, its complexity and cost increases. A report from Families USA, a health care advocacy organization, found that each year as much as $45 billion is wasted on unnecessary testing, inappropriate use of medications, redundant treatments, and avoidable hospital readmissions.14 If not managed, the effectiveness and efficiency of health care will decrease, and its cost will be unsustainable.15
Coordinated care is designed to manage a team of health care professionals.
Coordinated care (also known as case management) and disease management16 grew out of this situation, as new strategies to ensure the delivery of high-quality care and manage cost. They share a common goal, but they differ substantially in their perspective and scope.17
What Is Coordinated Care?
Coordinated care is designed to manage a team of health care professionals. It does not address a specific illness or condition.18 Instead, it ensures consistency and transparency across all providers involved with patient care (doctors, nurses, therapists, pharmacists, facilities, public and private insurance payers, etc.).19 Coordinated care also recognizes the patient as a functional member of the team.20
Role of the PCP
Central to the strategy is the patient’s primary care physician (PCP) in ambulatory care. The PCP is the linchpin of the team and is often the only team member with a comprehensive awareness of all aspects of the patient’s care. PCPs are in the unique position to identify conflicts between team members.
The PCPs have the biggest impact on controlling costs,21 as they control access to specialists, diagnostic tests, and procedures. It is interesting to note that insurance policies that do not require referrals from the PCP may actually undermine the effectiveness of coordinated care, as the patient can bypass the PCP and may not report the involvement of other health care professionals, such as independently consulted specialists.
In long-term care and post-acute care, however, the PCPs are involved less, if at all, and other care team members assume that central role. For example, in skilled nursing and long-term care, the attending physician may assume the PCP’s role. In post-acute care, a nurse or care manager may be the point person, while in long-term services and supports (LTSS), a case manager may play that central role.
What Is Disease Management?
In contrast to the broad approach of coordinated care, disease management is narrowly focused on specific chronic, and typically costly, conditions such as diabetes, heart disease, and COPD. Its primary purpose is to control costs while ensuring that patients receive the most appropriate and effective medical care for their condition.22
Disease management is generally offered by medical insurance companies and government health plans such as Medicare and Medicaid. Patients usually receive it through contracts with specialized independent third parties.
Coordinated care and disease management are not mutually exclusive. In fact, disease management can be, and usually is, a component of coordinated care.23
2.4 Care Planning and Coordination Models
Care coordination comes in three models: social-based, medically oriented or integrated. All models bridge health and supportive services. When successfully implemented, these models can foster good health outcomes and reduce costs.
Social models aim to provide resources and referral, screening and assessment, care planning, authorization of services, and a monitoring structure.
2.4.1 Social Models
Care coordination involves marshaling personnel and other resources needed to carry out all required patient care activities. It is often managed by the exchange of information among participants responsible for different aspects of care.24 Many provider agencies, health systems, integrated networks, and even payers coordinate the patient’s health care with social needs. This way, they ensure the patient receives the right services at the right time to improve care, promote independence, and reduce unnecessary services. Care coordination helps patients and families access and navigate complex health care delivery systems, facilitate communication among multiple providers, monitor changes, and arrange for, and schedule, services.
One review of case management literature concluded that there is professional agreement on the components common to most case management models. However, it found many variations in the way components are implemented, including outreach, screening and intake, comprehensive assessment, care planning, service arrangement, monitoring, and reassessment.25 Variations exist based on services’ location and purpose and case management programs’ focus and administration.
Social models aim to provide resources and referral, screening and assessment, care planning, authorization of services, and a monitoring structure.26 Although social models do not address medical care, they are important in supporting it. Better coordinated care that leverages community resources to align social determinants of health is needed; examples include housing, healthy food, and safe neighborhoods (Institute for Health Care Improvement, 2011). Originally, social models supported case management systems in managing home and community-based long-term care services.
Social models not only assess and authorize institutional, residential and in-home services but also can build linkages with health providers.27 They are common among the states. Because most states want to standardize program management, they contract with, or designate, an agency to administer the programs. Area agencies on aging, county social service agencies, or local field offices of state aging departments are most often designated.28
As the health care system evolves and the nation continues to make advances in treating chronic illnesses, care coordination has emerged as a necessary, if not essential, way to help people find the services they need to stay independent. Social models provide a framework for care management systems that enable people to formally coordinate services through a network of community-based long-term care programs and services. Using the right services at the right time enables people to manage their health and social needs, maintain their independence, and improve their quality of life.
2.4.2 Medically Oriented Models
The medically oriented model is a collaboration of care planning and coordination among an array of health care professionals and the patient. It strives to develop the most appropriate holistic treatment as the patient goes through his or her disease. The medical models ease the patient’s transition from the hospital to the community or facilitate the patient’s ability to stay in the community.29
Medical models strive to develop the best holistic treatment for the patient.
A key element in continuity of care planning is gathering patient medical history, either using technology or manually transferring assessments to ensure health care records are accurate. The degree of patient satisfaction and cost reduction determines the effectiveness of the medically oriented model.
In the medically oriented model, the primary care physician integrates the psychological, biological, and social benefits to meet the patient’s needs. However, the primary care physician typically focuses only on the physical nature of the disease.
Care planning and coordination is most effective when medical health records and assessment tools are readily available to follow the patient, making the transition organized and patient focused. A few assessments that support accurate communication when the patient moves from one setting to the next are mentioned below:
- The Universal Transfer Form contains clinical information about the patient that communicates their current medical status, ensures accurate continuity of care, and reduces medical error.
- The electronic medication list shares all current medications and treatments.
- SBAR (Situation, Background, Assessment, and Recommendation) is a tool that allows healthcare professionals to communicate standardized information, making reports concise, objective, and relevant to the patient’s needs.
- The Physicians Orders for Life Sustaining Treatment (POLST) is a valid medical order that becomes a part of the patient’s medical record, ensuring that his or her wishes are expressed and respected.
- Summary and Discharge Reports.
Access to patient history, assessments, and wishes provides confidence in determining the right orders, knowing how and when to follow up, and caring for the patient in any medical/community setting.30
Care planning and coordination of care provides insights to the care team, improves communication and efficiency among team members, and will increase the patient’s satisfaction with health care services. We should not believe that the medical model is only about doctors’ powers, but remind ourselves that patients are active participants. Using the medically oriented model in care planning and coordination will help foster relationships of trust among primary care provider, attending physician, or other clinicians in the case of long-term and post-acute care, and the patient.
2.4.3 Integrated Models
Integration of health care is not only a trend today, but also necessary for a prosperous quality of life (Salerno, 2015). As people develop new health concerns, or their conditions change or deteriorate, there is an increasing need for multiple levels of care in a number of different heath care settings, including the home and community and a broad array of social supportive services.
Integrated models combine medical and social support needs, and hence can have significant economic effect on the health care system.
However, trying to coordinate care when multiple care providers are treating different diagnoses or are offering treatment for the same diagnosis is a challenge. Patients should remain the focal point of the plan of care for the best and safest outcomes. How can each specialty provider communicate their patient’s needs to the other providers to give the patient better outcomes and quality of life? Health IT, including interoperable EHRs, health information exchange, and telehealth can facilitate this communication among providers.
There are many types of electronic systems available for Health Information Exchange. Many systems are not interoperable with each other, offering limited and one-way communication even within the same organization, let alone across provider organizations. As a result, care providers may conduct duplicate tests and prescribe unnecessary medications. Unnecessary drugs may include some on the “red flag” FDA regulated list, such as psychotropic, antidepressants, and controlled medications for anxiety.
Primary care physicians have the legal authority to write scripts for these drugs, but they do not have the extensive training in the drugs’ use that psychiatrists do. This allowed practice may contribute to additional medical complications, especially when the inappropriate medications are used to treat geriatric and adolescent patients with no care coordination in place. Lack of coordination and communication has its penalties, first and foremost to the patient, and to the failure of the health care system.
The Centers for Medicare & Medicaid Services (CMS) is beginning to reduce payments to practices that do not comply with various CMS initiatives. In 2012, CMS started imposing a penalty on physicians who do not meet e-prescribing (eRX) levels. The eRX penalty started in 2012 at 1% and increased to 2% in 2014.31 In 2015, CMS began imposing penalties on physicians and hospitals for not complying with electronic health record implementation standards, following up on “meaningful use” incentive payments for EHRs.
Providing the pathways through integrated models can have a significant economic effect on the health care system. For care planning and coordination to be truly successful, an affordable universal health information exchange system is needed.
3. Types of Care Planning and Coordination Technologies (non-mutually exclusive categories)
3.1 Care Planning and Coordination Tools
are plans are built on information from multiple sources, including information about the patient, their conditions and health concerns, goals, observations, the care team, interventions, and even living situations and availability of caregivers and/or social support network or services.
Enabling technologies include interoperability, structured and unstructured data from different sources, a terminology platform that can map between standard vocabularies and locally created content, health information exchange, information repositories, and application program interfaces.
Care planning and coordination tools involve the following:
Care Planning:
- Gathering information from different resources, including an extended care team from multiple provider organizations and potentially the patient/care recipient and their family.
- Reconciling and updating the information.
- Creating a care plan with person-centered health and/or support concerns, goals, preferences, observations, and care team, as well as care and support tasks and their timeline and/or review date.
When such a plan is created collaboratively with input from multiple caregivers and care providers, the process is called shared or collaborative care planning.
In this white paper and portfolio, CAST emphasizes the importance of shared care planning to better serve patients. Shared care planning can be especially helpful for those with multiple comorbidities, providers, and caregivers and various support needs, like the older adult population.
Care Plan Communication:
Sharing the care plan with other team members and potentially inviting them to update information or amend the plan.
Care Coordination:
- Assigning tasks to care team members and ensuring they accept critical tasks.
- Documenting and tracking the care plan’s execution and outcomes.
- Requesting a need to update information and amend the care plan.
Shared care planning and coordination tools can be classified into three categories:
- Shared care planning tools
- Care and case management tools, and
- Care coordination and communications portals/ tools.
3.1.1 Shared Care Planning Tools
Shared care planning tools accomplish at least one of the following tasks:
- Enable care team members to input information and help create the care plan.
- Share a draft care plan with assignments for other care team members to review.
- Allow care team members to provide input, accept assignments, and sign off on the plan.
Shared care planning tools allow multiple care stakeholders to help create a care plan collaboratively.
Shared care planning tools allow multiple care stakeholders to provide input and help create a care plan, rather than the traditional care planning approach where one provider, such as a primary physician creates the care plan. In shared care planning, each care team member has multiple opportunities throughout the process to provide input and accept specific assignments. These tools should enable all members of the care team to securely access and contribute information, according to their roles.
Patients, family members, other designated caregivers, and health care providers granted access by the patient should be able to initiate modifications and record progress related to care plans. These notations include new barriers to achieving goals and changes in circumstances or lifestyle.32
3.1.2 Care Management and Case Management Tools
3.1.2.1 Care Management Definition and Tools
Care management is defined as a set of activities whose objectives are to do the following:
- Assist patients and their support systems in managing medical and behavioral conditions to improve patients’ functional health status,
- Enhance coordination of care,
- Eliminate duplication of services, and
- Reduce the need for expensive medical services.
Care management occurs at various levels of the health care system, including at a population level, at a practice or panel level, and at the person or individual patient level. Because of the challenges that patients with chronic conditions present, care management programs often focus on a chronic condition such as heart disease, diabetes, or asthma.33
The role of health IT in care management is to support care management functions.
The role of health IT in care management is to support care management functions, including patient data capture, aggregation, analysis, and reporting. Electronic registries, electronic health records (EHR), telehealth, and remote patient monitoring are enabling care management to move from the health insurance company to the clinical practice.
For example, a primary care clinic using health IT is now able to quickly group patients by health condition and identify their unmet needs, enabling care managers to target their services appropriately for each patient and to identify any gaps in care and service for disease-specific populations. Other technologies, such as interactive voice recognition, enable patients to be alerted and encouraged to get needed services, while freeing up care managers for higher-level interventions to close gaps in care.34
3.1.2.2 Case Management Definition and Tools
The case manager’s role is broader than that of a health care manager. The case manager addresses the other social determinants of health and assists patients with things like housing, domestic violence, food assistance, etc. The Case Management Society of America defines case management as “a collaborative process of assessment, planning, facilitation, and advocacy for options and services to meet an individual’s health needs through communication and available resources to promote quality cost-effective outcomes.” 35
Case management tools can help an organization create and organize all patient/client cases. The technology-based case management tools help users easily navigate different cases, review and assign actions or tasks as needed, and keep a clear audit trail or history of actions on a case.
3.1.3 Care Coordination and Communications Portals/Tools
Care coordination and communication portals/tools make communicating the care plan to all care team members easier. These portals and tools allow all care team members to access care plan information to ensure the care plan is being followed through appropriately. The portal can also assign care tasks to external care parties.
3.2 Sources of Information
Care plans are built on information from multiple sources, including information about the patient, their conditions and health concerns, goals, observations, the care team, interventions, and even living situations and availability of caregivers and/ or social support network or services. The patient, family members, and caregivers may enter information, and other sources of information that may feed into or enlighten a care plan may include the following:
- Information systems
- Referral systems
- EHRs (including LTSS EHRs)
- Data repositories and health information exchange entities
- Telehealth and remote patient monitoring (RPM) technologies
- Medication management technologies
- Functional assessment and activity monitoring technologies
- Wellness systems, etc.
3.3 Enabling Technologies
3.3.1 Interoperability
Interoperability means that two disparate systems are able to communicate with one another to exchange data. To end users and many in the industry, interoperability means all products work together seamlessly. Unfortunately, this is an expectation that not even the most highly integrated suite of components in a product fully achieves yet.
Experts estimate that 80 to 90% of the data in any organization is unstructured.
3.3.1.1 Structured and Unstructured Data
Structured data refers to any data that resides in a fixed field within a record or file. Each field has a description associated with it and sometimes a specific data range. Structured data has the advantage of being easily entered, stored, queried, and analyzed. At one time, because of the high cost and performance limitations of storage, memory, and processing, relational databases and spreadsheets using structured data were the only way to effectively manage data. Anything that couldn’t fit into a tightly organized structure would have to be stored on paper in a filing cabinet.36 Hence, structured data is often not only human, but also machine readable.
Unstructured data refers to information that doesn’t reside in a traditional row-column database. Unstructured data files often include text and multimedia content. Examples include e-mail messages, word processing documents, videos, photos, audio files, presentations, webpages, and many other kinds of documents. Note that while these sorts of files may have an internal structure, they are still considered “unstructured” because the data they contain doesn’t fit neatly in a database. Experts estimate that 80 to 90% of the data in any organization is unstructured. And the amount of unstructured data in enterprises is growing significantly — often many times faster than structured databases are growing.37
3.3.1.2 Relevant Vocabularies and Standards
Vocabulary standards are playing a key force in enabling interoperability of patient data. Meaningful Use may be accomplishing what hasn’t happened before – a set of rules everyone will follow to allow patient data to flow between EHR systems, delivery networks, and regional organizations. Whether the vocabulary standard is a classification system, terminology, controlled vocabulary, or nomenclature, a terminology server can provide a range of services to use and manage these complex entities.38
To achieve interoperability within and across disparate health care IT systems, both free text and structured clinical information need to be synchronized across various applications. A terminology platform delivers a set of services and functions to map, manage, mediate, and manipulate terminologies for use and re-use in clinical applications.
A terminology platform supports sharing within as well as across applications. A terminology platform can map:
- Between standard vocabularies,
- Between locally created content and standard vocabularies, and
- Between sets of locally created content.
This mapping supports standardized descriptions of clinical findings, patient observations, diagnoses, and interventions, allowing consistently entered information across care settings and by care providers. The EHR benefits by having a terminology platform that can ensure valid coded terms have been used.39 Currently, health IT systems in use support a limited number of vocabularies, including SNOMED-CT, LOINC, and RxNorm.
The HL7 Consolidated Clinical Document Architecture C-CDA R2.x includes a set of section and entry level templates to support the exchange of Care Plan CDA documents, including implementation of Case Management/Disease Management Care Plan CDA illustrated in this webpage.40
HIE can facilitate access to clinical data to provide safe, timely, efficient, and patient-centered care.
3.3.2 Health Information Exchange
Health information exchange (HIE) entities provide the capability to electronically move clinical information among and between disparate health care information systems and maintain the meaning of the information being exchanged. The goal of HIE is to facilitate access to and retrieval of clinical data to provide safe, more timely, efficient, effective, equitable, and patient-centered care. Public health authorities also use HIE to assist in analyzing the health of populations.41
In terms of transfer of care, as patients make the transition from one care setting to another (such as from hospital to provider community), HIE services allow the documentation from one care setting to be easily accessed from the next.
3.3.3 Information Repositories
An information repository is a collection of interrelated information maintained across a network on multiple servers. It creates a unified resource for anyone connected with the system to access when they need information. Numerous organizations use information repositories to handle their data and may network with others to share material as necessary. The underlying information technology needs to be very robust to handle the volume of information and frequency of requests. This term can also refer to a specific kind of data management.
The information repository deposits relevant data along with meta-information on a regular basis. Users can run a query to find material relevant to their interests. Repositories may include a variety of types of information, including images, video, and text. Users may be able to narrow searches by type to find specific materials. Passwords and other security measures often limit access to protect the information’s integrity and limit abuses of the system.42
3.3.4 APIs
An application program interface (API) is code that allows two software programs to communicate with each other. The API defines the correct way for a developer to write a program that requests services from an operating system (OS) or another application. APIs are implemented by function. The documentation of the application being called usually describes the required syntax.
Typically, APIs are released for third-party development as part of a software development kit (SDK) or as an open API published on the Internet. If the applications are written in different languages or have been written for different platforms, middleware can provide messaging services so that the two applications can communicate with each other.43
Today, many APIs are developed to improve interoperability and facilitate interfacing, data integration, and information exchange among information systems, including health IT systems.
4. Potential Uses of Care Planning and Coordination Technologies

The general approach to care planning and coordination involves organizing a patient’s care needs and personal preferences to be communicated among care teams. Targeted care coordination plans guide the care team to ensure the patient is receiving the right care, in the right place, at the right time to improve outcomes and reduce avoidable complications. Conceptually, it all makes sense; however, in reality, coordination and collaboration among various health care teams has been difficult to achieve.
With the emerging value-based payment landscape, it is clear that aligning care teams to share data and coordinate care plans across the entire continuum of care is essential. This coordination will achieve strong performance in quality of care measures and reduce the cost of care. Moreover, engaging the patient and their family members and coordinating with family caregivers as part of the extended care team is paramount to improving outcomes and reducing cost. The transition period between hospital discharge and post-acute follow-up care, sometimes known as the “hand off” segment in the continuum of care, has been well documented as fragmented and can increase costs by $25 billion to $45 billion annually.44
Along with changes to health care reimbursement, the baby boomers who have a strong preference to age in place are having an impact. As the baby boomers become Medicare eligible, there is a great need for chronic disease management programs. Statistics indicate that baby boomers have more chronic diseases than their predecessors.45 Additionally, chronic conditions account for 93% of all Medicare spending.46 Using the community’s readmission rates and evidence-based care strategies, senior living providers can leverage their expertise as collaborative strategic post-discharge partners to hospitals, Accountable Care Organizations (ACO), and other providers.
Today, the ability to share data with collaborative partners is vitally important to health care providers. The evolution of mobile connected care coordination platforms that offer the capability to share care plans is crucial not only in care transitions, but also in supporting care continuity between patients at home and health care providers.
Applications and uses of care planning and coordination may include the following:
- Patient education and support of self-management
- Pre- and post-acute chronic disease management
- Support and stabilization of post-acute patients
- Shared care and transitions of care
- Coordination of support services for older adults and other populations to maximize outcome, support independence, and minimize the impact of social determinants of health and associated health care costs.
Connected virtual care coordination platforms that capture patient-generated health data give clinicians the opportunity to evaluate trends and mitigate potential patient risks.
In conjunction with the ability to include patient generated data, the ability to communicate with, and educate, patients at home is an important feature for care management. Mobile care platforms that incorporate secure messaging, virtual visits, and the ability to send educational resources at the time of need enables clinicians to build relationships with patients at home and engage them in their personal health.
To be successful in the outcome-based payment era, health care providers need innovative person-centered mobile health solutions that enhance their ability to:
- Identify the need for early interventions and proactive care for transitional care,
- Provide chronic disease management, and
- Offer wellness strategies.
Health care reform has provided a golden opportunity for senior living providers to engage in shared care planning and coordination.
In essence, health care reform has provided a golden opportunity for senior living providers to engage in shared care planning and coordination. Successful health outcomes require moving beyond the office visit. Health care providers need collaborative outside partners in order to achieve sustainable care metrics. Forward-thinking senior living providers can affect care delivery models at home by leveraging interactive connected care platforms and their skill sets to provide virtual support at home.
5. Potential Benefits of Care Coordination and Care Planning Technologies

There are many studies on the impact of case management, care management, and care coordination on health outcomes and cost. A 2009 systematic review of the effects of case management for frail older adults and individuals with chronic conditions revealed that two out of 11 randomized controlled trials showed evidence of reduced utilization and cost associated with case management. None of the remaining nine studies showed any increase in utilization or cost.47 In another study, Lemmens et al. reviewed the evidence of chronic care management on COPD patients. The review generally showed positive impact on quality of life and hospitalizations, but not on emergency department visits.48
However, fewer studies focus primarily on the effects of electronic care planning and coordination technologies. A stringent literature review contributed by Ostrovsky et al. focused on randomized controlled trials (RCT), the gold standard in clinical research, revealed that such studies were very limited. Consequently, there is lack of strong evidence of the benefits of these technologies. Nevertheless, care coordination technology still holds promise to achieve the Triple Aim. The review also emphasized the need for more RCT evaluation studies. One potential contributor to the limited peer-reviewed evidence for outcomes associated with care coordination technologies may be the diversity of feature needs by end users.49 For example, in a 2016 environmental scan for care coordination technology, no existing suitable care transition tool was found. Instead, the scan revealed the value of creating a tool to fulfill the specific care transition needs of patients, family members, and providers.50
Given the lack of evidence and relative immaturity of care planning and coordination technology, a more appropriate evaluation may be a needs assessment of this technology class. Richardson et al. conducted one using semi-structured telephone interviews with 28 participants from three Patient-Centered Medical Homes (PCMHs) in the United States. The researchers identified five areas in which health IT can improve care coordination in PCMHs:
- Monitoring patient populations,
- Notifying clinicians and other staff when specific patients move across care settings,
- Collaborating around patients,
- Reporting activities, and
- Interoperability.51
One of the few non-randomized but controlled studies encountered comprehensively evaluated the impact of an electronic open-source adaptive case management system, called Linkcare®, on integrated care services in patients with chronic conditions with varied severity. Linkcare® supported advanced case management with shared-care plans across health care tiers and offered integration with provider-specific electronic health records. The study showed that Linkcare® successfully contributed to the deployment of the four integrated care services:
- It facilitated long-term sustainability of training effects in rehabilitation and active life style,
- It showed significant positive outcomes in enhanced care,
- It reduced on average five in-hospital days per patient with a 30-day re-admission rate of 10% and
- It enhanced community-based quality forced spirometry testing.
The study also identified key challenges for regional deployment of personalized care and strategies to overcome them.52
In what follows, we will review some of the literature we encountered that showed promise for care coordination technologies, categorized by the area of potential impact.
5.1 Improved Health Outcomes
One randomized controlled trial (RCT) evaluated the impact of mobile phone text messages and calls on ambulatory care management in patients with arterial hypertension. Posnenkova et al. found that at the end of the one-year study period, 77% of patients from the active care management group had achieved the goal blood pressure level, which was more than five times higher goal achievement rate than that in the traditional ambulatory care management group (P<0.001).53
In another study, Marek et al. evaluated the effect of a medication management technology and nurse care coordination on the health status of 414 frail older adults discharged from Medicare-certified home health agencies.54 The patients were randomized into one of three arms and received either no intervention, a care coordination intervention with no technology, or a care coordination intervention with a medication management technology. Throughout the -one-year study, participants with care coordination had significantly better health status outcomes than those in the control group, but adding the medication management technology to nurse care coordination did not result in better health status outcomes.
5.2 Hospitalizations, Hospital Length of Stay, and Emergency Department Visits
An evidence-based review of electronic tools for health information exchange and care coordination, conducted by the Ontario Health Quality, identified four randomized controlled trials and seven observational studies that showed moderate quality evidence of a reduction in hospitalizations, hospital length of stay, and emergency department visits after an electronically generated laboratory report with recommendations based on clinical guidelines was implemented. The evidence showed no difference in disease-specific outcomes; there was no evidence of a positive impact on process-of-care indicators or measures of efficiency.55
HIE access was associated with a decrease in hospital admissions, in head CT use, body CT use, and laboratory test ordering.
Another study evaluated the financial impact of health information exchange (HIE) in emergency departments (EDs). The study reviewed access to HIE data by 12 EDs over a 13-month period. It showed that HIE data were accessed in approximately 6.8% of ED visits across 12 EDs studied. In 11 EDs directly accessing HIE data only through a secure web browser, access was associated with a decrease in hospital admissions relying more on print summaries. HIE access was also associated with a decrease in hospital admissions and statistically significant decreases in head CT use, body CT use, and laboratory test ordering. The study concluded that HIE data were accessed in approximately 6.8% of ED visits across 12 EDs studied.56
In a retrospective study, Matiz et al. evaluated the impact of information technology tools on the outcomes of children with asthma in the medical home. A registry was established for children aged four to 18 years with an ICD-9 code for asthma. Changes to the electronic health record included modifications to notes, care plans, and orders. A retrospective analysis of emergency department and in-patient utilization for a cohort of patients was conducted from July 2009 through June 2013. Of the study population (n = 1217), 65% had a classification of asthma severity, and 63% were risk-stratified. Seventy percent had a control assessment at least once. Care plan use increased from 5% to 22%, and enrollment in care coordination increased from 0.1% to 4%. After three years, there was a statistically significant reduction of emergency department and inpatient admissions for asthma. The study concluded that implementation of information technology tools for care coordination was associated with improved asthma outcomes.57
5.3 Prolonging Independence and Reducing Long-Term Care Costs
In a recent study, Rantz et al. evaluated the impact of sensor monitoring combined with registered nurse coordinator on length of stay (LOS) of residents in TigerPlace, an Aging In Place community. The study showed that residents living with sensors were able to reside at TigerPlace 1.7 years longer than residents living without sensors, suggesting that proactive use of health alerts facilitates successful aging in place. Health alerts, generated by automated algorithms interpreting data from sensors embedded in the environment, may enable care coordinators to assess and intervene on health status changes earlier than is possible in the absence of sensor-generated alerts. Comparison of LOS without sensors TigerPlace (2.6 years) with the national median in residential senior housing (1.8 years) may be attributable to the RN care coordination model at TigerPlace. Cost estimates comparing cost of living at TigerPlace with the sensor technology vs. nursing home reveal potential savings of about $30,000 per person. Potential cost savings to a Medicaid-funded nursing home (assuming the technology and care coordination were reimbursed) are estimated to be about $87,000 per person.
6. Potential LTPAC Provider Business Models
6.1 Medicare Coverage
Medicare covers care planning and coordination under three types of services: Care Plan Oversight, Chronic Care Management, and Transitional Care Management.
6.1.1 Care Plan Oversight
A care plan oversight (CPO) is when a physician supervises a patient receiving complex and/or multidisciplinary care as part of Medicare-covered services provided by a participating home health agency or Medicare-approved hospice. CPO services require complex or multidisciplinary care modalities involving the following:
- Regular physician development and/or revision of care plans,
- Review of subsequent reports of patient status,
- Review of related laboratory and other studies,
- Communication with other health professionals not employed in the same practice who are involved in the patient’s care,
- Integration of new information into the medical treatment plan, and/or
- Adjustment of medical therapy.
The CPO services require a physician to supervise a patient, recurrently, for 30 or more minutes per month. To bill for CPO, the physician must provide some services that do not count toward the 30minutes. These services include, but are not limited to, the following:
- Time needed to discuss adjusting medication or treatment with the patient, or his or her family or friends;
- Time spent by staff getting or filing charts;
- Travel time; and/or
- Time spent telephoning prescriptions into the pharmacist, unless the telephone conversation involves discussions of pharmaceutical therapies.
Implicit in the concept of CPO is the expectation that the physician has coordinated an aspect of the patient’s care with the home health agency or hospice during the month for which CPO services were billed. The physician who bills for CPO must be the same physician who signs the plan of care.
Doctors, nurse practitioners, physician assistants, and clinical nurse specialists may bill for care plan oversight.
Nurse practitioners, physician assistants, and clinical nurse specialists, practicing within the scope of state law, may bill for care plan oversight. These non-physician practitioners must have been providing ongoing care for the beneficiary through evaluation and management services. These non-physician practitioners may not bill for CPO if they have been involved only with the delivery of the Medicare-covered home health or hospice service.58
Medicare uses two Healthcare Common Procedure Coding System (HCPCS) codes, G0181 and G0182, to define and pay for CPO. The definition of G0181 is “physician supervision of a patient receiving Medicare-covered services provided by a participating home health agency (patient not present) requiring complex and multidisciplinary care modalities involving regular physician development and/or revision of care plans, review of subsequent reports of patient status, review of laboratory and other studies, communication (including telephone calls) with other health care professionals involved in the patient’s care, integration of new information into the medical treatment plan and/or adjustment of medical therapy, within a calendar month, 30 minutes or more.” G0182 describes the same service for a patient in a Medicare-approved hospice.59
6.1.2 Chronic Care Management
Under the 2015 Medicare Physician Fee Schedule (PFS), starting in January 2015, physicians became able to receive $40.39 per month per qualifying patient for care coordination management (CCM) furnished by a clinical staff provided under the supervision of the physician or other qualified clinician.
Physicians may supervise and bill for clinical staff providing care coordination management (CCM).
Services include +20 minutes non-face-to-face planning and management for patients with two or more chronic conditions who provide a written consent to receive CCM. These services may include medication titration or care management based on telephone interactions, asynchronous teleconsultation services (using secure messaging or biometric remote monitoring), and the like, but they must be documented in a Certified EHR system. Documentation must include the patient’s demographics, problems, medications, and medication allergies, and it must create structured clinical summary records.
A comprehensive person-centered care plan based on a physical, mental, cognitive, psychosocial, functional, and environmental (re)assessment is required. So is an inventory of resources—a comprehensive plan of care for all health issues. The care plan must do the following:
- Provide the patient with a written or electronic copy of the care plan and document its provision in the medical record,
- Ensure the care plan is available electronically at all times to anyone within the practice providing the CCM service, and
- Share the care plan electronically outside the practice as appropriate.
The comprehensive person-centered care plan typically includes, but is not limited to, the following elements:
- Problem list,
- Expected outcome and prognosis,
- Measurable treatment goals,
- Symptom management,
- Planned interventions and identification of the individuals responsible for each intervention,
- Medication management,
- Community/social services ordered,
- A description of how services of agencies and specialists outside the practice will be directed/coordinated, and
- Schedule for periodic review and, when applicable, revision of the care plan.
The new Current Procedural Terminology (CPT) code for CCM services is 99490. Examples of conditions eligible for reimbursement include, but are not limited to, these:
- Alzheimer’s disease and related dementia
- Arthritis (osteoarthritis and rheumatoid)
- Asthma
- Atrial fibrillation
- Autism spectrum disorders
- Cancer
- Chronic Obstructive Pulmonary Disease
- Depression
- Diabetes
- Heart failure
- Hypertension
- Ischemic heart disease
- Osteoporosis
Eligible providers include physicians, certified nurse midwives, clinical nurse specialists, nurse practitioners, and physician assistants.60 Please see the following white paper, Providing and Billing Medicare for Chronic Care Management, for a detailed explanation of the CMS Rule.61
6.1.3 Transitional Care Management
Also under the Physician Fee Schedule (PFS), Medicare started in January 1, 2013, paying for two CPT codes (99495 and 99496) that are used to report physician or qualifying non-physician practitioner transitional care management (TCM) services for a patient after the following:
- A discharge from a hospital, SNF, or Community Mental Health Center (CMHC) stay;
- Outpatient observation; or
- Partial hospitalization.
The patient must be discharged to his or her community setting, such as a home, domicile, rest home, or assisted living. The requirements for TCM services include the following:
- The services are required during the beneficiary’s transition to the community setting following particular kinds of discharges.
- The health care professional accepts care of the beneficiary post-discharge from the facility setting without a gap.
- The health care professional takes responsibility for the beneficiary’s care.
- The beneficiary has medical and/or psychosocial problems that require moderate or high complexity medical decision making.
- The 30-day TCM period begins on the date the beneficiary is discharged from the inpatient hospital setting and continues for the next 29 days.
Physicians and several non-physician practitioners may furnish transitional care management services.
Health care professionals who may furnish TCM services include physicians (any specialty) and the following non-physician practitioners (NPPs) who are legally authorized and qualified to provide the services in the state in which they are furnished:
- Certified nurse-midwives (CNMs),
- Clinical nurse specialists (CNSs),
- Nurse practitioners (NPs), and/or
- Physician assistants (PAs).
For more details, please see Medicare’s fact sheet on Transitional Care Management Services.62
6.2 Medicaid Coverage
Medicaid and the Children’s Health Insurance Program (CHIP) provide health coverage to nearly 60 million Americans, including children, pregnant women, parents, seniors, and individuals with disabilities. To participate in Medicaid, federal law requires states to cover certain population groups—called mandatory eligibility groups—and gives them the flexibility to cover other population groups—called optional eligibility groups. States set individual eligibility criteria within federal minimum standards. Medicaid coverage is based on financial and other non-financial eligibility criteria that are used in determining Medicaid eligibility. To be eligible for Medicaid, individuals need to satisfy federal and state requirements regarding residency, immigration status, and documentation of U.S. citizenship. These criteria vary by state.63
States are encouraged to use innovative payment methods to incorporate telehealth technology.
CMS requires that reimbursement for Medicaid-covered services, including care planning and coordination, must also satisfy federal requirements of efficiency, economy, and quality of care. With this in mind, states are encouraged to use the flexibility inherent in federal law to create innovative payment methodologies for services that incorporate telehealth technology.
Some state Medicaid managed and integrated (Medicare and Medicaid) care plans have requirements for care coordination.64
6.3 Program of All-Inclusive Care for the Elderly (PACE)
PACE (Program of All-Inclusive Care for the Elderly) is a Medicare and Medicaid program that helps people meet their health care needs in the community instead of going to a nursing home or other care facility. PACE organizations provide care and services in the home, the community, and the PACE center. They have contracts with many specialists and other providers in the community to make sure that patients get the care they need.
PACE focuses on individual enrollees, who have a team of health care professionals working with them and their family to make sure they get the coordinated care they need. Many PACE participants get most of their care from staff employed by the PACE organization in the PACE center. PACE centers meet state and federal safety requirements.65
Pull quote: PACE providers have flexibility in covering traditionally uncovered benefits, which may encourage the adoption and use of care planning and coordination, as well as other, health information technologies.
Because PACE providers operate under a capitated payment model and are at risk for all care costs, including hospitalization and nursing home costs, they have a vested interest in controlling costs and flexibility in covering traditionally uncovered benefits. This setup may encourage PACE providers, more than their traditional fee-for-service counterparts, to adopt and utilize care planning and coordination solutions, as well as other aging services technologies including functional assessment, activity monitoring, telecare, telehealth, and medication management technologies to deliver health care and supportive services.
6.4 Private Health Insurance Coverage
There is no single widely accepted standard for private insurance coverage of care planning or care coordination services. Some insurance companies value the benefits of care planning and coordination and will reimburse a wide variety of services. Others have yet to develop comprehensive reimbursement policies, so payment for care planning and coordination may require prior approval. Likewise, different states have various standards by which their Medicaid programs will reimburse care planning and coordination expenses. Also as with Medicaid, states set regulations for care planning and coordination reimbursement by private insurers.
In addition to private health insurance, emerging private models like Life Plan Communities (formerly Continuing Care Retirement Communities (CCRCs)) and Life Plan at Home may cover care planning, care management, and care coordination services to prolong their residents’ or enrollees’ independence and reduce their cost.
6.5 Potential Affordable Care Act (ACA) Opportunities
The Affordable Care Act (ACA) is shifting the health care system in the U.S. away from the traditional fee-for-services to a pay-for-performance system. Moreover, CMS is moving to reimburse Medicare Certified Home Health based on a value-based purchasing model instead of a prospective payment model. This shift is starting to eliminate the misalignment of incentives inherent in traditional Medicare, Medicaid, and private insurance programs.
The ACA includes many provisions that might encourage adoption of care planning and coordination technologies and services.
There are many provisions and models in the ACA that would benefit from, provide opportunities to cover, and encourage the adoption of care planning and coordination technologies and services.66 The act created the Center for Medicare & Medicaid Innovation (CMMI), which is tasked with exploring new care delivery and payment models and initiatives67 that do the following:
- Use more holistic, patient-centered, and team-based approaches to chronic disease management and transitional care.
- Improve communication and care coordination among care providers.
- Improve care quality and population health while reducing growth in expenditures.
The act puts explicit emphasis on the use of health information technology (health IT), including care planning and coordination technologies, in health homes for enrollees with chronic conditions, the Independence at Home Demonstration, and the use of technology in new state options for long-term services and supports.68
These initiatives include the following:
- Hospital Readmission Reduction Program (HRRP).69
- ACOs.70
- Bundling of Payments models, of which the following two are relevant to LTPAC providers:
LTPAC providers bring a significant value for hospitals, physician groups, payers, and ACO partners by providing the following services:
- Rehabilitation and skilled nursing facilities provide post-discharge/post-acute patient rehabilitation.
- Skilled nursing facilities, assisted living facilities, continuing care retirement communities, housing with services, and home health agencies provide post-acute patient stabilization and sub-acute chronic disease management.
- LTPAC provides holistic person-centered care, including support services.
- LTPAC offers lower-cost care settings than hospitals.
These new care delivery and payment models will enable LTPAC providers who use technologies, like care planning and coordination technologies, to derive revenue sources from strategic partners. The following white paper, The importance of home and community-based settings in population health management, offers some key questions LTPAC providers should discuss with their acute care partners.
Private payers may be another payment source.
6.6 Private Pay
Another payment source for care planning and coordination services may be private payers or out of pocket. As mentioned above, Medicare covers some transitional care management within 30 days of hospital discharge to the home and/or for chronic care management. When the Medicare coverage period expires, or is not available, providers may offer these services, if clients would benefit from such a program as private pay covered out of the patient’s or family’s pocket.
6.7 Standard of Care and Other Payment Sources
Long-term post-acute care (LTPAC) and community health providers, special population agencies, self-pay and self-insured organizations, and others, especially not-for-profits, may offer or cover an array of care planning, coordination, and/or management services. These services may be covered by grants or offered as standard of care. The organization may absorb the cost, or different revenue sources, including charitable contributions, may cover it.
6.8 Return on Investment (ROI) of Care Planning and Coordination
Return on investment (ROI) represents the ratio of the net gains relative to the initial investment over a certain period of time. Subsequently, ROI can be expressed in the following equation:
![]()
As discussed above, care planning and coordination deliver various benefits, including potential financial savings to different stakeholders, including patients and/or their families, payers, care providers, etc.
Pull quote: ROI depends on the care delivery model, the payment/reimbursement model, the technology, and costs.
However, the financial savings and ROI depend on a number of factors, including the care delivery model, the payment/reimbursement model, the technology, and of course costs. The first and most important step in calculating ROI is to consider the different stakeholders, identify the investors, and calculate the gains and savings netted/accrued to each investing stakeholder under each particular care delivery and payment model. When calculating ROI, one should only include the gains that accrued to that particular stakeholder minus all expenses, relative to that stakeholder’s own investment/cost. Often the reduction of hospital days is erroneously included in the providers’ ROI, which is not true under the traditional fee-for-service reimbursement model and can be misleading; such a reduction usually accrues to the payer.
6.8.1 ROI to Patients and/or their Families
ROI to patients and/or their families can be calculated as follows:
![]()
For private pay patients and their families, for example, the financial gains of care coordination lie in prolonging independence by maintaining health, which may prevent disability, and avoiding the need to move into assisted living or skilled nursing facilities. These benefits are significant. The gains may also include savings in co-pays for recurring hospital visits, and of course a higher quality of life, which is difficult to quantify. The patient’s and family’s expenses are the monthly out-of-pocket of private care services, plus any co-pay for the occasional physician office visit, lab tests, and prescriptions.
6.8.2 ROI to Payers
ROI to payers can be calculated as follows:
![]()
For dual Medicare and Medicaid eligible patients who are nursing home eligible, for example, the financial gains of care coordination under a Medicaid Managed Care program that accrue to program depend on keeping patients in their own homes with home health, home care, and other supportive services. Otherwise, the managed care would be liable for the costs of nursing home room and board. Managed care’s investment is the monthly rate of care coordination, as well as home- and community-based supportive services aimed at keeping the individual independent.
Additional savings, like reductions in hospitalization and hospital readmission costs, may accrue to Medicare or the managed care plan. Consequently, such savings or gains should be correctly attributed.
6.8.3 ROI to Care Provider
ROI to care providers can be calculated as follows:
![]()
The care provider who makes investments in information and communications technology infrastructure, care planning and coordination technology, and who offers care coordination and management services, may reap the following benefits:
- Lower costs in delivering the same services, including staff efficiencies and staff travel costs (if the payer covers the remote services, rather than just the in-person visit).
- Higher reimbursements/payment from the payer or strategic partner in terms of incentive payments for avoiding more costly care settings, procedures, events, or penalties.
For example, an LTPAC provider partnering with a physician group ACO to manage a chronically ill patient population can potentially get a percentage of the incentives or shared savings payments the ACO receives from the payer for reducing hospitalizations and hospital readmissions, which can be significant for certain populations.
- The LTPAC provider’s net gain is the sum of all gains accruing to the LTPAC provider in staff efficiencies, increased referrals from the ACO, traditional fee-for-service payments for eligible services, and additional incentive payments received from the ACO, minus the costs of care coordination technology and actual costs of services delivered.
- The physician group ACO’s ROI is the portion of the payer’s incentive payment that they get to keep plus any additional fee-for-service payments due to more frequent office-based services, minus the actual costs of services they deliver (for example, in medication reconciliation), relative to the portion of incentives they pass through to the LTPAC provider.
A contrast is a partnership between an LTPAC provider and hospital under the traditional fee-for-service model. For example, the LTPAC provider may help its hospital partners reduce 30-day readmission rates for pneumonia, congestive heart failure, and heart attack patients, helping the hospital avoid Medicare’s payment penalties under the Hospital Readmissions Reduction Program.
The hospital may contract with and pay the LTPAC provider a percentage of the penalties saved for delivering better coordinated care that reduces 30-day readmissions for patients discharged from the hospital after being admitted for pneumonia, congestive heart failure, or heart attack.
- The LTPAC’s net gain is again the sum of all gains accruing to the LTPAC provider in staff efficiencies, increased referrals from the hospital, traditional fee-for-service payments, and additional payments received from the hospital, minus the costs of care coordination technology and actual costs of services delivered.
- The hospital’s ROI is the portion of avoided penalties it gets to keep, plus any additional fee-for-service payments it gains for more referrals due to improved quality ratings, minus the actual costs of services the hospital delivers, relative to the portion of avoided penalties it passed through to the LTPAC provider, plus any additional costs incurred for staff time in care coordination, medication reconciliation, or health information exchange.
An online tool can help calculate ROI for person-centered care coordination.
6.8.4. Online ROI Calculator
Once individual investors have been clearly identified, an estimate of the ROI to the different stakeholders can be calculated. The SCAN Foundation has recently published a white paper on making the business case for person-centered care with instructions for using an ROI calculator they developed.73
This return on investment (ROI) calculator is designed to quantitatively assess the business case for person-centered care (PCC) programs that serve older adults with chronic conditions and functional limitations. PCC programs are ones where individuals’ values and preferences are elicited and, once expressed, guide all aspects of their health care, supporting their realistic health and life goals. This type of care is achieved through a collaborative relationship and decision-making process among the person, their chosen supports, and their medical and social service providers. As discussed in detail above, the business case for PCC involves weighing the costs of offering this approach to care against the benefits expressed in dollar terms. Benefits accrue principally in the form of avoided medical utilization, but also potentially in the form of higher revenues.
The ROI calculator has a number of practical features:
- Risk Stratification: The population that is suitable to receive PCC can be segmented into high and moderate risk categories. The ROI will be likely higher (i.e., a higher percentage) for the segment that is at higher risk for medical utilization. The calculator can show how limited the offering must be if a specific return were being sought. Potential Revenue from PCC: The calculator allows for PCC program offerings to incorporate possible revenue enhancements in addition to the more probable benefits resulting from reducing costs.
- Slider Bars: This feature allows the user to compute instantaneous “what-if” calculations by changing values of inputs and immediately viewing these new inputs’ influence on the ROI.
- Flexibility in Expressing Variables: All variables can be entered by the user in terms of their convenience – per person, per month, or per year. Hospital admissions, for example, are generally reported on an annual basis whereas encounters with a social worker or nurse practitioner are often expressed on a monthly basis. The calculator automatically converts rates and volumes, no matter how expressed, into a common per member per month (PMPM) measure.
- Scenarios: This feature allows ROI comparisons across different programs as well as varied constellations of input values. For example, the user can create optimistic and pessimistic scenarios and compare the results. Sometimes even the pessimistic scenario can yield an acceptable result for the ROI.
- Accounting for Uncertainty: Admittedly, some key determinants of the ROI are not known with certainty. Therefore, a “Monte Carlo” simulation that accounts for uncertainty with respect to the magnitudes of key variables is an optional part of the tool. This simulation recognizes this uncertainty and displays accordingly a reasonable range of results for the ROI rather than a single deterministic value. The tool also quantifies the strengths of the separate influences each variable has on the resulting ROI.
- Other Metric – Payback Period: In addition to the ROI result, the calculator displays the payback period – defined as the number of months the PCC program would need to operate (assuming a positive operating margin) for any initial investment to be recouped. This metric may be useful for programs involving substantial up-front launch costs.
- Threshold Analysis: The tool provides the ability to conduct threshold analysis, whereby the user can query the calculator on questions such as the following: What is the maximum amount that can be spent on PCC so that the program does not lose money? Or for a given cost of delivering PCC, how effective must it be in reducing certain events (e.g., hospital readmissions) in order to generate a required (hurdle) level of ROI?
To access the calculator tool, go to The SCAN Foundation.
7. Planning for and Selecting Appropriate Care Planning and Coordination Technology
“It’s simple but revolutionary to think of individual medical care in the context of a plan, with specific goals and tracking mechanisms. The health care experience changes fundamentally, particularly for a person with complex challenges … if all members of the care team are engaged in the success of that plan.” 74
Care planning and coordination technologies have become increasingly important to the health care system in order to provide continuity of care along the care continuum.
Implementing these technologies will require teams to understand the strategic goals and vision of the organization and its care partners.
Implementing care planning and coordination technologies is complex and will require a teamwork approach to understanding the strategic goals and vision of the organization and its care partners. Planning will require evaluating the organization’s team and operational readiness, along with any partners’ preparedness to assist in an individual’s care. These technologies can be an important tool to manage numerous medical needs from various health professionals within the patient’s circle of care. “Without a strong communication link between care providers, negative consequences such as poor health outcomes, errors in treatment, increased readmissions to hospitals, wasted resources, and dissatisfied patients may result.” 75 Communication and teamwork are the fundamental elements in the selection, planning, and implementing of care planning and coordination technology.
7.1 Understanding the Population, Issues, Care Settings, Needed Services, and Care Partners
[[{“attributes”:{},”fields”:{}}]]
A significant increase of the senior population over the next 20 years is expected. This population will have individuals with multiple, complex, and chronic health conditions, including Alzheimer’s disease and other types of dementia. One-third of those 85 and older will be diagnosed with a form of dementia. The loss of memory and other intellectual abilities will interfere with the activities of daily living for many seniors throughout the United States and the world. These issues will make it difficult for health care systems and providers to deliver quality care without some type of care coordination system and the use of technology.
Care partners must use technology that can support mutual decision making of a diverse group whose members operate on different timescales and seldom meet.
Care settings for seniors can include their own or relative’s home, independent living communities, assisted living, adult family homes, rehab centers, nursing homes, and more. As an individual transitions in life with their medical needs, he or she will require services in a variety of settings. These services can include home health, home care, monitoring, medication assistance, and support with the activities of daily living. As a person ages, “Transitions can occur at many different times and places in a person’s health care journey, and might include: referrals from a person’s family physician to specialist care, admission into a hospital, discharge out of the emergency department or hospital, and admission to a long-term care facility from the person’s home.”76
Care partners will not only include the physician (PCP and medical specialists), but also health care providers from a variety of settings, such as clinical staff from hospitals, long-term care facilities, therapists, home care workers, and family and friends, to mention a few. Care partners must develop a successful team and with the use of technology capable of supporting the collaborative, mutual consensus decision making of a diverse group whose members operate on different timescales and seldom if ever meet as a full group. Shared care planning and coordination tools should ideally cater to this and be capable of connecting and supporting the entire extended care team and the care network as a whole.
7.2 Planning for Care Planning and Coordination Solutions
7.2.1 Visioning and Strategic Planning
Visioning and strategic planning are key elements of successful organizations. When considering care planning and coordination technologies, it is imperative to align with the organization’s corporate plans and establish clarity on the organizational goals and overall strategy.
To be successful in the planning process, a strategic planning workgroup should be established and include the following stakeholders: care planning and clinical team members, IT staff, corporate or administrative representatives, physician and community health partners, supportive services partners, and patient/family members. Communication will be vital. The group will need to establish clear goals and objectives, define high-level technology requirements, and develop a plan of action, milestones and/or performance measurements. Together, group members must determine if care planning is realistic in terms of partnerships, collaboration, and resources.
7.2.2 Organizational Readiness Assessment
Planning for and implementing a care planning and coordination technology program is a complex and time consuming endeavor. It requires an entire care team, time, resources, and dedication. An integrated care team brings together both internal operations as well as additional care partners who deliver services that the target population needs and that the organization does not offer.
The process should start with reviewing the current care planning and coordination processes and tools, their advantages, where they may be failing, and where additional partners, information, resources, or technology solutions may be needed.
Together, care partners should envision an optimized coordination and communication process. Then the assessment should focus on the ideal shared care plan, and the resources and requirements all care partners need to carry out this plan. This list includes technology requirements for care planning coordination tools; types of data needed and their sources; integration, interfacing, interoperability, and information exchange needs; the existing IT infrastructure that would be needed to support the new approach; and the existing and additional competencies needed.
Designating individuals that are accountable, qualified, and available to carry out these responsibilities is a first step in evaluating the state of an organization’s preparedness. Establishing the provider partners’ commitment will help influence success in initiating a care planning and coordination technology program.
7.2.2.1 Available Technology Solutions
It is important to learn about the types of care planning and coordination technologies available, how they function, their uses and benefits, their high-level network requirements, and the connectivity they require.
With the ideal shared care plan/planning and coordination in mind, consider the type(s) of care planning and coordination solutions needed.
Things to consider include the following:
- Does the technology need allow you to collaborate with others on creating the shared care plan? Does it need to assign care tasks to members of the extended care team? Does it need to support acknowledgement, acceptance, rejection, or scheduling by a remote extended care team member?
- Does the care planning and coordination tool need to support care plan oversight, facilitate chronic care management of certain common chronic conditions, and support transitional care management?
- What areas of health, care, social, and logistic support needed by the target population should the technology tool support?
- Does the solution need to support communications with and engagement of certain members of the extended care team outside the organization? If so, who and how?
Sections 3, 4, and 5 of this white paper represent a great introduction to care planning and coordination technologies.
7.2.2.2 Available Data
Based on the initial assessment, and the ideal care plan and coordination process, consider the data that would be needed to create and periodically update integrated care plans. Then the data can be organized into these categories:
- Data readily available to the organization and/or care partners,
- Additional data essential to have in the care plan, and
- The source of that data.
A primary data source would be the patient’s electronic health records. These records will provide much of the needed information for compiling the essential data. Other sources may include medication adherence records, telehealth data, data from behavioral and activity monitoring systems, and/or data from safety monitoring technology.
An understanding of what information is necessary from each partner organization’s standpoint will be essential to establishing a successful care planning and coordination program.
7.2.2.3 Additional Data Needed and Sources
It is also important to focus on the types, and sources, of data that is currently not readily available to the provider but that would be essential or extremely beneficial for successful care planning and coordination. Family members and other providers, including people that patients identify as part of their care team or social support network, will be able to provide additional data or information. These people will be a primary source for information and patient care on a day-to-day basis. Consider the format, modality, and frequency of getting this data in a way that does not add to the burdens of the extended care team.
7.2.2.4 Interoperability/ interfacing Capability
Once all needed information and data, their format and their sources, have been identified, one should consider all the interfacing, integration, interoperability, and information exchange needs. In this step, consider vendors that have implemented interoperability standards, have application program interfaces (APIs) to other systems, have successfully integrated with other systems, and/or have demonstrated exchanging the types of information needed for your program. Please keep in mind that sometimes you may not find one system that meets all your requirements, and you may need to work with integration engines.
7.2.2.5 IT Infrastructure
Selecting the appropriate care planning and coordination solution will depend on an organization’s IT infrastructure and needs. Typical options include the following:
- Purchasing and locally hosting the care planning and coordination software on-site at the organization’s data center.
- Purchasing the software and hosting it in a third party’s data center.
- Having the vendor host and offer its own Software as a Service (SaaS).
Each has pros and cons depending on an organization’s size and current IT infrastructure.
Some things to consider when evaluating these options are as follows:
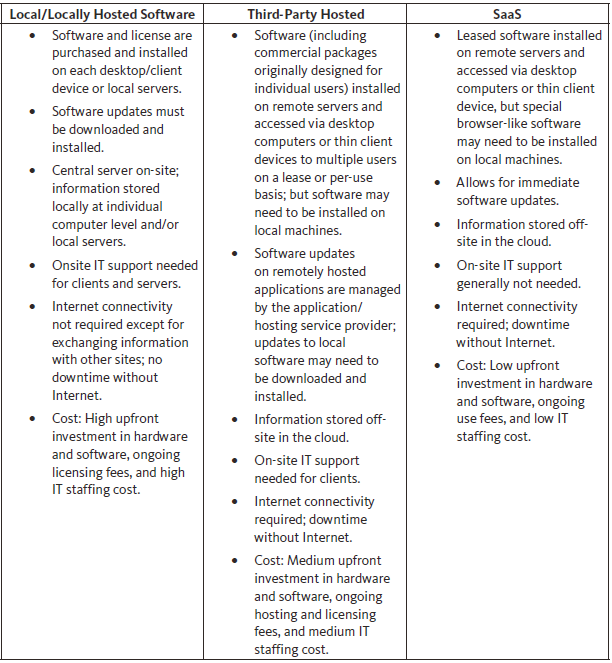
Consider the implications of the type of solution on the existing IT infrastructure, including network, Internet access, speed, and bandwidth. Remember that you need to start your project implementation with updating your IT infrastructure.
7.2.2.6 Staff Competencies and Availability
Basic foundational competencies such as intellectual, interpersonal, leadership, organizational, and self-management skills are needed to perform any job. These five competencies will be the groundwork to a successful care team. You should consider the roles of care team members, their required education/certification/training, competencies, and preferred skill sets to successfully launch and sustain the care planning and coordination program envisioned. All partner organizations will need to assess staff members’ availability and competencies. The partners then can determine if existing staff members have the skills needed to contribute to the goals and success of the care planning and coordination technology program, or whether the partners need to hire. Organizations should offer multiple training options directly related to the employees’ job descriptions and caregiver needs.
7.2.2.7 Considerations for Resident/ Patient and Family-Facing Solutions
7.2.2.7.1 Assessment of Issues/Needs
The issues and needs of a resident/patient will need to be examined by looking at patient compliance. Involving the patient as an active contributor to the care plan is an important step to achieving patient engagement in, and compliance with, the plan.
However, not all patients want to be involved in the planning process. The Strengthening Assessment and Care Planning Guide produced by the Department of Health in Victoria, Australia, notes that some patients are not motivated to set goals and may resist being involved in developing their care plan. The guide indicates that care planning is not for everyone and that goal development tends to work best for the following:
- Patients who are motivated toward achieving or participating in something specific.
- Patients who have had a recent change (or decline) and are motivated to act.
- Patients of any age or functional ability with the capacity for functional improvement or restorative gains. 77
7.2.2.7.2 Assessment of Competencies/Abilities
The success of care depends on who is responsible for overseeing the care planning and coordination. Families will need to discuss who has the ability and competencies to maintain, monitor, and help create and update information, and potentially to follow up. Staff will need to assess patient competencies, and the family and patient need to agree on who is the best person to develop and maintain an effective process. Families will need to determine if this type of care and coordination is practical given abilities and time constraints of those involved. A designated lead person (patient or family member) will need to be established prior to implementing the program. This step is especially important when caring for patients with cognitive issues or other limitations.
7.2.2.7.3 Assessment of Personal Preferences
The health care consumer (resident/client/patient) will need to consider what is most important at the time a service of care planning and coordination technologies is offered. The care team will want to consider the following questions:
- What do I hope to achieve?
- What we can do to achieve it?
- Who will be responsible?
- What is the expected outcome?
- What are the barriers and challenges?
7.2.2.7.4 Ability to Pay
For most Americans, the ability to pay for health care is becoming more difficult every day. Cost of care and payment resources have become a critical policy issue. Government and private insurers have examined alternative models of payment that may or may not participate in a care planning and coordination program. Each health care consumer will need to evaluate payment methods and determine the affordability of his or her own care.
7.2.2.7.5 Provider Services and Responsibilities
Care providers will need to review with the patient and personal care team the common challenges and pitfalls that can hinder the proper development and implementation of care planning and coordination technologies. In addition, providers will need to identify the appropriate person or persons to maintain the care plan and communicate the patient’s needs if those needs are not being met. If done well, the patient and care team will experience success and a positive experience in the care planning and coordination program.
7.2.2.8 Operating Environment (including Applicable Federal and State Regulations)
The type of software solution will most likely be directly influenced by the type of operating environment required to meet your business needs. Understanding and defining organizational, provider, and family access will help determine the most effective operating environment. Consider the following items:
- Required access to the system remotely from any web-enabled device.
- Provider access, including partner providers.
- Family portal access.
- Storing all information securely behind firewall protection.
Review security issues and understand the transmission requirements of data and information. Organizations should ensure that data obtained and shared is done in compliance with all the applicable Health Insurance Portability and Accountability Act (HIPAA) Privacy and Security Rule requirements. Under the new HIPAA Omnibus Rule, which became effective in March 2013, covered entities’ business associates are now directly liable for compliance with certain HIPAA Privacy and Security Rules requirements. These measures include “a mechanism to authenticate,” “a mechanism to encrypt and decrypt electronic protected health information (ePHI),” and “policies and procedures to protect ePHI from improper alteration or destruction.”
It is important to consider unique organizational needs and applications to ensure the appropriate operating environment is chosen.
7.2.3 Operational Planning
7.2.3.1 Project Team
Successful implementation of care planning and coordination technologies relies on engaging a wide array of stakeholders in the planning effort. The most successful care planning and coordination programs incorporate the program into the organization’s day-to-day operations and involve all staff in the program to some degree. Since care planning and coordination technology is enabling a new care delivery model, most staff will need to be involved, including executive leadership, clinical teams, technical representatives, finance, operations, and marketing/business development. Several outside partners will need to join the extended care team. These partners include, but are not limited to, physicians, therapists, home health aides, and the patient’s family and friends. Getting all of these groups on board with a clear set of goals, timelines, resource requirements, and deliverables will lead to success.
7.2.3.2 Goal Setting
Defining the care planning and coordination program goals is critical to measure success. Each organization will have different ideas of what success looks like based on strategic goals and internal operations. Before starting a care planning and coordination program, the organization should set a clear series of goals and metrics.
Keep in mind that goals should be measurable and routinely reported on within your operations. The fundamentals to setting goals are to ensure that they are SMART goals:
- Specific.
- Measurable.
- Attainable.
- Realistic.
- Trackable.
Setting both short-term and long-term goals for the care planning and coordination program is highly recommended. The program will naturally change and progress over time. Organizational goals set at the program’s start will likely be different six to 12 months post implementation. Care planning and coordination program goals should be evaluated continuously and updated as programs change. It is also important to understand that a new program will have the ability to achieve several major goals during its initial adoption.
Goals for each organization should be unique and may incorporate ideas from the following categories:
Clinical Outcomes
- Improved integration/coordination of care.
- Reduction of hospitalizations.
- Reduction of hospital readmissions.
- Improved health and wellness.
- Improved self-management skills.
Satisfaction Outcomes
- Improved patient satisfaction scores.
- Improved provider satisfaction scores.
- Higher employee satisfaction and retention.
- Increased trust from the patient.
- Increased feeling of security in the home environment.
Operational Outcomes
- Improved partnerships with physicians and other health care providers.
- Increased staff and partnership productivity/efficiencies.
- Focus on wellness and intervention and needs.
- Attraction of new talents.
- Better positioning and market advantage.
Financial Outcomes
- Reduction in readmissions.
- Increased productivity.
- Increased community partnerships.
- Increased market share/referrals.
- Increased occupancy.
- Increased opportunity for new lines of business.
Be sure to define outcome measures that will help in evaluating the program’s success in the short and long term. After determining program goals, capture and discuss baseline data during the program’s planning sessions. Periodically review and update these goals and metrics throughout the planning and implementation process.
7.2.3.3 Program Design
Care planning and coordination programs should be designed with the organizations’ short- and long-term goals in mind to help ensure success. Additional items that should influence the program design include care coordination, collaboration, and communication to enhance patient care and outcomes with the care team and other providers along the continuum of care.
Each program’s design should always consider how to align objectives, strategies, and technical plans with care partners by using care planning and coordination technologies and the EHR as an information source and communications facilitator. Be sure to share experiences from other similar organizations to assist in strategies to build a care planning and coordination program within the organization or strengthen an already existing one. Please see the companion case studies that CAST is collecting.
Before starting any program, clearly define the new model of care and prepare staff with training and support plans.
7.2.3.4 Operating Model, Workflow, and Change Management
Implementing a new technology program does not just mean adding technology into an existing care model. On the contrary, care models themselves change because patient care planning and coordination is being conducted differently. This distinction is particularly significant for the clinical care model.
Before starting any program, clearly define the new model of care, care planning, care coordination, and communication in conjunction with care partners. Prepare staff with training and support plans. To gain the most benefit, ensure care planning and coordination technology is used as a tool for changing care delivery and workflows, both inside the organization and with outside partners, and not simply an add-on. Adding care planning and coordination technology, or any other technology for that matter, without assessing and redesigning processes, workflows, and communications to take advantage of the technologies’ capabilities and efficiencies will likely fail to produce the anticipated benefits.
7.2.3.4.1 Patient Population
At the earliest stages of planning, identify the patient population the organization wants to reach with care planning and coordination technologies. As part of this process, ensure there is a process for identifying and enrolling patients and gathering their consents. Demonstrating the value of care planning and coordination and making sure that patients understand their care will be improved, not diminished, is at the heart of the consent process.
7.2.3.4.2 Business Model: Expenses and Revenue Sources
Consider the care delivery and payment model(s) being proposed for the care planning and coordination program. Identify all expenses, including technology infrastructure, connectivity, care planning and coordination system expenses, installation, troubleshooting, maintenance and support, change management, training, clinical services, and support. Identify all the revenue sources (private pay, payer, strategic partner), and carefully calculate the organization’s ROI, as well as the other stakeholders’ (please see section 6).
7.2.3.5 Positive Approaches to Coordinated Care Planning
While the practice of coordinated care planning involves several challenges, the literature on this topic outlines several positive approaches that can assist with, and hopefully improve, the care planning process. These approaches include the following:78
- Identify someone to be responsible for the plan’s coordination and maintenance. When plan updates are made, there needs to be a system in place to distribute the updated care plan to the patient and the patient’s care team.
- Involve the patient in all aspects of the care planning process to increase the patient’s likelihood of complying with the recommended treatments. When possible, involve the family, patient advocate, or primary caregiver in the planning process as well.
- Ensure the patient understands the purpose of the care plan and the planning process. Prepare the care plan using language that is easy to understand; use plain language and avoid health care jargon. This can be particularly challenging if the patient is illiterate or does not understand the care planner’s language. A translator or family member may need to be present to ensure the patient understands the care plan. Pictures or diagrams may also be helpful to the patient.
- Make the care plan available in a format that the patient can access easily. Ensure the patient has a copy of the plan and ask him or her to keep a copy in a place that is easily accessible.
- Take into account the issues that are important to the patient and reflect those issues through the patient recovery goals.
- Facilitate seamless transitions by sharing information and responsibility among providers and patients.
- Think outside the box, beyond traditional treatments. For example, patients may benefit from coordinating services with community resources outside of the health care system, such as financial resources like welfare or food stamps, educational resources, support groups, or support programs like Meals on Wheels.79
7.2.3.6 Technology Review and Selection
Once an organization has completed the visioning and strategic planning exercise, assessed organizational readiness, assembled the project team, set the project’s goals, and designed the program, then the team needs to develop a set of detailed requirements to use as criteria to review and select the appropriate care planning and coordination technology solution.
Setting and Focus:
The planning process would help identify key requirements that should include the following:
- The care setting(s) where the organization wants to deploy the care coordination solution; this should be the primary setting for the targeted population (home health, skilled nursing facility, housing with services, etc.).
- The target population and the types of care and social support issues the organization wants to manage and coordinate.
- The partner organizations/settings needed and/or secondary settings to coordinate with; this step is especially important for care coordination during transitions of care.
The criteria should inform the types of care planning and coordination systems that may help the organization achieve its goals.
System Type:
System types include the following:
- Shared Care Planning Tool
- Care/Case Management Tool
- Care Coordination and Communication Portal/Tool
Care Plan Components – Patient Summary:
In addition, the above information would inform the types of data needed in the care plan’s patient summary section, which may include the following:
- Demographics
- Advanced Directives
- History of Past Illness
- Family History
- Social History/Risks
- Allergies
- Medications
- Immunizations
- Medical Equipment
- Vital Signs
- Functional Status
- Cognitive Status
Care Plan Components – Health Concerns, Goals, Instructions and Interventions, Review, Care Team:
In addition, the above information would help you decide other types of information you need to include in the care plan. This information may include the following:
- Health Concerns
- Goals
- Instructions and Interventions
- Review
- Care Team (Formal and/or Informal)
Sources of Information, Interfacing and Integration:
The discussion of the data types needed and the information sources will inform the system’s interfacing and integration needs. These may include the following:
- Referral Systems
- EHRs
- Telehealth/RPM
- Medication Management Technologies
- Functional Assessment and Activity Monitoring Technologies
- Wellness Systems
- HR Systems
- Information Systems
- Patient-Generated Data
Program Development and Vendor Support:
The available resources, capabilities, and expertise in program design and operationalization would inform the type and level of development and support you would need from the prospective vendor. These may include the following:
- Program Development (planning, business model templates, etc.)
- Comprehensive Care Planning and/or Management Services
- Clinician Engagement Services
- Patient Education Program/Services
- Patient Engagement Program/Services
- Care Provider/Care Manager Engagement
- Family Engagement Program/Services
Status Reports and Communication with Care Team, Access:
Other high-level differentiating factors include the care planning and coordination backend system’s ability to produce the following:
- Customizable Reports
- Analytic Reports
- Ability to Schedule Automatic Reports
The following may gain access to the status reports:
- Client/Resident/Patient’s Physician
- Client/Resident/Patient’s Nurse/Other Licensed Clinician
- Care Manager/Professional Caregiver
- Client/Resident/Patient/User/Self
- Family
Alerts:
Another important feature is generating immediate urgent alerts and sharing them with interested parties, including the following:
- Client/Resident/Patient’s Physician
- Client/Resident/Patient’s Nurse/Other Licensed Clinician
- Care Manager/Professional Caregiver
- Client/Resident/Patient/User/Self
- Family
Legal and Regulatory Requirements:
Of course legal and regulatory requirements are important. The two most important legal and regulatory requirements relevant to shared care planning and coordinating technologies include compliance with the following:
- The Health Insurance Portability and Accountability Act (HIPAA), which set national standards to protect individuals’ medical records and other protected personal health information (PHI).
- The Health Information Technology for Economic and Health (HITECH) Act, which sets additional standards to demonstrate meaningful use of security technology to ensure the confidentiality, integrity, and availability of protected electronic medical records and electronic personal health information (ePHI).
Programs must comply with HIPAA and the HITECH Act.
Hardware and Software Requirements:
Finally, hardware/software requirements that could guide the selection process include how software is offered:
- Local Model, which means that it needs to be installed on servers local to the care provider, or
- Third-Party Hosted Model/Software as a Service Model (SaaS), where the software is hosted somewhere else and the provider pays licensing and hosting fees or pays for usage, as opposed to maintaining local servers’ infrastructure.
Other important hardware and software requirements include remote access functionality support, off-line functionality support when running Third-Party Hosted or SaaS software, and mobile device support, such as for smartphones and tablets.
Use the CAST Shared Care Planning and Coordination Online Selection Tool to narrow down the selection to a few shortlisted candidate systems and vendors that meet the must-have high-level requirements.
In the CAST Shared Care Planning and Coordination Selection Matrix, we outline many additional options and detailed features and functionalities. These details will help drill down into these shortlisted products and narrow the selection to a list of two or three vendors who can be invited to submit a response to a request for proposals (RFP).
During the RFP process, providers are encouraged to interview prospective vendors and engage many staff in the interviews and product evaluation: front staff, nursing and medical directors, care managers/ coordinators, and representatives from management, finance, and IT teams. Please check provider case studies with the vendors, including those collected by CAST, and conduct appropriate due diligence including reference checking. In addition, providers may want to use the LeadingAge CAST/Technology Listserv to ask peers about the shortlisted products and their experience with these vendors.
7.2.3.7 Implementation
The implementation and planning phase takes the information gained by the assessment phase and begins to develop answers to the who, how, and when questions. During this phase, executive steering committee members are identified and a project charter is created. Enough time should be set aside for this phase, as it is involved and detailed.
This stage includes agreeing upon project scope and goals, developing a communication plan, and identifying the project team members who will actually implement the system. The project implementation team should be a patient-centered interdisciplinary team consisting of, at a minimum, physicians, nurses, pharmacists, care managers, IT staff, representatives of care partners, and residents/patients and families. A project plan identifying milestones, resources, tasks, and timeline comes from this phase.
The focus should include the patient’s journey through care settings.
Project tasks include mapping clinical and business processes and developing new processes and procedures. The scope should not be confined to the care planning and coordination processes. The implementation team’s focus is patient-centered and should include the patient’s journey. The patient’s journey through care settings needs to be part of the mapping.
Contingency planning is part of the overall plan; the team must assess and identify potential risks throughout the project and deal with them quickly. Most often, risk is not going to severely impact the project, but when a risk that could impact the project’s timeline, budget, or goals appears, the steering committee should be made aware to make decisions.
7.2.3.8 Post-Implementation Monitoring
It is important to provide continuous monitoring of any program. Monitoring validates the program, tracks improvement, and identifies any new problems that may occur. Measuring the program’s quality will provide an opportunity to establish its positive impact on the organization, consumers and any partners. If post-monitoring does not show significant differences in care planning and coordination for those individuals served, the organization will need to rethink the program.
8. Care Planning and Coordination Matrix Components
Summary: The Care Planning and Coordination Selection Matrix has 18 sections to help organizations narrow the possible shared care planning and coordination products.
CAST’s Care Planning and Coordination Workgroup, consisting of providers, vendors, and consultants, compiled a list of Care Planning and Coordination products that serve the LTPAC market, as well as a list of functionalities and capabilities that would help providers choose the product that best fits their business line and functional requirements.
Each of the Care Planning and Coordination vendors then received the opportunity to complete a self-review of the workgroup’s pre-determined questions. Some of these vendors chose not to participate. Those who participated then could nominate a case study from a provider’s perspective on the use of the vendor’s Care Planning and Coordination product.
The Shared Care Planning and Coordination Matrix includes the following sections:
Business Line/Care Applicability
Business line/care applicability illustrates the various business lines to which the functional assessment and activity monitoring product is applicable, including the following:
- Acute Care Settings (Physicians’ Offices, Emergency Department, Hospitals, Attending LTPAC Physician).
- LTPAC and Other Settings (Home Health/Home Care, Hospice, Housing with Services, Community-Based Programs, Adult Day Care/Senior Centers, Assisted Living Facilities, Acute Rehab Facilities, Long-Term Acute Care Hospitals, Long-Term Care Rehab Facilities, Skilled Nursing Facilities, Intermediate Care Facilities, Intellectual Disabilities/Mental Retardation/Developmental Disabilities (ID/MR/DD) Facilities, Life Plan Community (Formerly CCRC), Program of All-Inclusive Care for the Elderly (PACE), Accountable Care Organizations (ACO)/Integrated Delivery Networks (IDN), Multiple Site Integration).
System Type
System type illustrates the different product types, including the following:
- Shared Care Planning Tools (Input Information and Participate in the Creation of the Care Plan from External Care Team Members, Share Draft Care Plan with Assignments for Review, and Sign Off by Care Team (Provided Input and Acceptance of Assignment).
- Care/Case Management Tools.
- Care Coordination and Communication Portal/Tools (Communicate Care Plan and Assign Care Tasks to External Care Team Members).
Care Plan Components – Patient Summary
This category includes the options for the following care plan components and whether or not the data is structured (machine readable) or non-machine readable, the standard for structure (if applicable), and the source of the data:
- Demographics
- Advanced Directives
- History of Past Illness
- Family History
- Social History/Risks
- Allergies
- Medications
- Immunizations
- Medical Equipment
- Vital Signs
- Functional Status
- Cognitive Status
Care Plan Components – Health Concerns, Goals, Instructions and Interventions, Review, Care Team
This category includes the options for the following care plan components and whether or not the data is structured (machine readable) or non-machine readable, the standard for structure (if applicable) and the source of the data:
Health Concerns
- Chief Complaint
- Current Health Problems
- Others
Goals
- High-Level Goals
- Low-Level Goals
Instructions and Interventions
- How to Care for the Care Recipient’s Condition
- Instructions Specific to Care Recipient’s Home
Review
- Deadlines for Reviewing Outcomes
- Make Adjustments Based on Review
Care Team
- Formal Care Team
- Informal Care Team
Sources of Information, Interfacing and Integration
This category includes the following options:
- Referral Systems
- EHR (including LTSS and Pharmacy EHRs)
- Telehealth and Remote Patient Monitoring (RPM) Technologies
- Medication Management Technologies
- Functional Assessment and Activity Monitoring Technologies
- Wellness Systems
- HR Systems
- Information Systems
- Patient-Generated Data
- Other
- Notes Standards
Program Development and Support Offered
This category includes options for the following:
- Program Development (Planning, Business Model Templates, Workflows, Change Management, etc.)
- Comprehensive Care Planning and/or Management Services
- Clinician Engagement Services
- Patient Education
- Patient Engagement
- Care Provider/Care Manager Engagement
- Family Engagement
- Other (Please List)
Front-End Hardware Unit Patient/Client/Resident/User Interface & Communications
This category includes the following options:
- Login Modality, Please list if applicable (e.g., Scan Card, PIN)
- Touch Screen
- Audible Prompts
- Visual Prompts
- Haptic Prompts
- Low Vision Support
- Customizable Questionnaires
- Thresholds Are Customizable
- Branching Logic Based on User’s Responses
- Communications Modality (Plain Old Telephone System (POTS) Line, DSL Internet Connectivity, High-Speed Internet Connectivity, Wi-Fi Connectivity, Cellular Connectivity, Minimum Internet Connectivity Speed Required)
Hardware and Software Requirements – Front End
These requirements list the required desktop/laptop specifications for Software-Only Solutions, including requirements for the following:
- Minimum Processor Speed, Hard Drive Storage, RAM requirements if applicable
- Operating System (OS) – Windows
- Operating System (OS) – Apple
- Operating System (OS) – Unix/Linux
Other features compared include the following:
- Network Specifications
- Wireless Specifications
- Modern Browser Support
- Minimum Internet/Bandwidth Specifications
- Miscellaneous Software/Applets Needed (i.e., Citrix)
- Miscellaneous Reporting Specifications (i.e., Crystal Reports)
- Scalability
- Local Model
- Hosted Model
- Software as a Service Model (SaaS)
- Remote Access
- Off-Line Functionality
- Support Ability to Store/Handle Attachments (Insurance card, Historical Notes, etc.)
- Available for Lease
- Available for Purchase
Lastly, mobile options are listed as the following:
- Cellular Carriers that Support Solution
- Mobile OS – Android
- Mobile OS – Blackberry
- Mobile OS – iOS
- Mobile OS – Unix/Linux
- Mobile OS – Windows and/or
- Mobile-Optimized Interface (through dedicated app or mobile-optimized webpages)
Finally, we added a tab for Additional Notes on hardware and software requirements.
Front-End Unit Support
This category includes the following options:
- Educational Self-Management Materials (On-Screen Educational Self-Management Material, Self-Management Educational Audios, Self-Management Educational Videos)
- Front-End Unit Multi-Language Support (English, Spanish, Mandarin, Cantonese, Korean, Russian, French, German, Hindi, Urdu, Portuguese, Arabic, Hebrew, Other (please specify)
- Remote Updates
- Remote Configuration Capability
- Status Reports, Communication with Care Team, Access
This element includes whether reports/records can be the following:
- Customizable Reports
- Analytic Reports
- Ability to Schedule Automatic Reports
Communication with Care Team using the following methods (Alerts, Secure Messaging, E-Mail, Direct Messaging, Video Conferencing, Other)
Report Access Provided to the Following External Parties (Client/Patient’s Physician, Client/Patient’s Nurse/Other/Licensed Clinician, Client/Patient/User/Self, Care Manager/ Professional Caregiver, Family, Other)
Alerts
This category includes the following options:
- Alerts Can Be Sent to the Following External Parties (Client/Patient’s Physician, Client/Patient’s Nurse/Other Licensed Clinician, Client/Patient/User/Self, Care Manager/Professional Caregiver, Family, Other)
- Alerts Sending Modality (Pager, Telephone, Voice Messages, E-Mail, Text Message, Other)
Program Support Services
- This category includes options for the following:
- Equipment Delivery/Pickup
- Site/Home Installation
- IT/Network Troubleshooting & Support
- Front-End System Setup
- Front-End System Customization
- Back-End System Setup
- Back-End System Customization
- On-site Staff Training
- Online Staff Training
- On-site User Training
- Online User Training
- Equipment Cleaning
- Equipment Refurbishing
- Other
Interoperability, Interoperability Standards, and Certification
This section begins with type of interoperability and exchange capabilities supported, which include the following:
- None, Export Data Only, Import Data Only, or Bi-Directional Data Import and Export
- This section also includes options for the following:
- Supported Interoperability Standards (HL7 Personal Health Monitoring Report, Other)
- Back-End HER/PHR Certification ((2014 ONC-ATCB Certification (Complete (please provide link); Modular (please provide link); No)Plan on pursuing ONC’s proposed voluntary certification?)
Care Planning/Coordination Supportability (Only Pertains to Vendors Offering Care Planning and/or Care Coordination Services)
This category includes options for the following:
- Phone Support–No, Yes (limited hours), Yes (24 hours)
- Web Support–No, Yes (limited hours), Yes (24 hours)
- E-Mail Support
- Listserv and/or Usergroup
- Online Training
- On-site Training
- Other
Technical Supportability
This category includes options for the following:
- Phone Support–No, Yes (limited hours), Yes (24 hours)
- Web Support–No, Yes (limited hours), Yes (24 hours)
- E-Mail Support
- Listserv and/or Usergroup
- Online Training
- On-site Training
- Other
- Warranty Information (Length of Product Warranty, Parts, Parts & Labor, Parts and In-Field/On-Site Labor)
Legal/Regulatory/Cyberliability
This area touches on the following:
- FDA Clearance/ Listing – Cleared, Listed (This category may include Medical Device Data System (MDDS)), Pending, or None
- FDA Classification (Class I, Class II, etc.)
- HITECH
- HIPAA
- Security – List HIPAA & HITECH Act Requirements Met
- List Applicable Regulatory Requirements Met
- Provide a Link to Company’s Cyberliability Policy
- List Any Other Legal Requirements
- Provide Link to Sample Contract
Hardware and Software Requirements –Back End
These requirements list the required desktop/laptop specifications for Software-Only Solutions, including requirements for the following:
- Minimum Processor Speed, Hard Drive Storage, RAM requirements if applicable
- Operating System (OS) – Windows
- Operating System (OS) – Apple
- Operating System (OS) – Unix/Linux
Other features compared include the following:
- Network Specifications
- Wireless Specifications
- Modern Browser Support
- Minimum Internet/Bandwidth Specifications
- Miscellaneous Software/Applets Needed (i.e., Citrix)
- Miscellaneous Reporting Specifications (i.e., Crystal Reports)
- Scalability
- Local Model
- Hosted Model
- Software as a Service Model (SaaS)
- Remote Access
- Off-Line Functionality
- Support Ability to Store/Handle Attachments (Insurance Card, Historical Notes, etc.)
- Available for Lease
- Available for Purchase
Lastly, mobile options are listed as the following:
- Cellular Carriers that Support Solution
- Mobile OS – Android
- Mobile OS – Blackberry
- Mobile OS – iOS
- Mobile OS – Unix/Linux
- Mobile OS – Windows and/or
- Mobile-Optimized Interface (Through dedicated app or mobile-optimized webpages)
Finally, we added a tab for Additional Notes on hardware and software requirements.
Company’s Experience and Viability
This area includes the following:
- Number of Years in Business
- Release Date of Current Version
- Number of Patients Served
- Core Customer Base/Focus of Line of Business
- Links to Additional Case Studies
The last section of the matrix is dedicated to the following:
- Strengths
- Areas for Improvement
- Ongoing Development
- References
9. Acknowledgement of Contributors
9.1 Contributing Writers
Andrey Ostrovsky, Care at Hand
Avrill Salcedo, The Francis E. Parker Memorial Home, Inc.
Cathy Guttman, Medocity
Dushwantie Loricka, The Francis E. Parker Memorial Home, Inc.
Gloria Walsh, The Francis E. Parker Memorial Home, Inc.
Kay Loricka, The Francis E. Parker Memorial Home, Inc.
Lisa Slater, The Francis E. Parker Memorial Home, Inc.
Lynette Ladenburg, LeadingAge Washington
Majd Alwan, LeadingAge CAST
Marcy Salzberg, The Francis E. Parker Memorial Home, Inc.
Michael Wallach, The Francis E. Parker Memorial Home, Inc.
Michael Yannotta, The Francis E. Parker Memorial Home, Inc.
Natalie Macaro, The Francis E. Parker Memorial Home, Inc.
Scott Code, LeadingAge CAST
Yolanda Golebiowski, The Francis E. Parker Memorial Home, Inc.
9.2 Workgroup Members
Andrey Ostrovsky, Care at Hand
Camille Roussel, National Lutheran Community
Candace LaRochelle, eHealth Data Solutions
Carmel Roques, Keswick
Cathy Guttman, Medocity
Debi Sampsel, UC College of Nursing
Doc DeVore, MatrixCare
Dusanka Delovska-Trajkova, Ingelside
Dushwante (Kay) Loricka, The Francis E. Parker Memorial Home, Inc.
Elizabeth Knight, Align
James Rosenman, FairView
Janice Oldmeadow, Philips
JJ Johnson, Cornell Communications
John Mabry, Align
Kian Saneii, Independa
Kim Speidel, National Church Residences
Lynette Ladenburg, LeadingAge Washington
Mark Anderson, Eldermark
Michael Matteo, The Village at Unity
Mike Yannotta, The Francis E. Parker Memorial Home, Inc.
Nancy Stoddard, The New Jewish Home
Olga Jewusiak, Caremerge
Patrick Lyon, Medtronic
Peter Kress, ACTS Retirement Communities
Sandrine Sauvage-Mack, LV Health Solutions Inc.
9.3 Participating Care Planning and Coordination Vendors
Seventeen vendors, including 9 CAST Partners, Supporters and Business Associates participated in the Shared Care Planning and Coordination Portfolio. These included:
Align, John Mabry
Philips, Janice Oldmeadow
PointClickCare, Ricardo Meirelles
MatrixCare, Doc DeVore
NetSmart, Jeremy Mercer
CAST Business Associates participating included:
Caremerge, Olga Jewsiak
Eldermark, Mark Anderson
Other Participating Vendors included:
CareTree, Carl Hirschman
ecoSoft Health, Jay Fruin
eTransX, Richard Taylor
Kno2, Dane Meuler
LivWell Health, Len Bargellini
Medocity, Cathy Guttman
Open Placement, Justin Usher
The Right Place, Katherine Chambers
10. References and Resources
1. Alex Baker, Kelly Cronin, Patrick Conway, Karen DeSalvo, Rahul Rajkumar, Matthew Press. (2016). Making the Comprehensive Share Care Plan a Reality. https://catalyst.nejm.org/making-the-comprehensive-shared-care-plan-a-reality/
2. http://www.ahrq.gov
3. Short, A., Mays, G. & Mittler, J. (2003). Disease management: A leap of faith to lower-cost, higher-quality health care? Center for Studying Health System Change. Retrieved from https://www.mathematica-mpr.com/insights
4. Traver, A. (2013). The promise of care coordination: Transforming healthcare delivery. Retrieved fromhttp://familiesusa.org/sites/default/files/product_documents/Care-Coordination.pdf
5. Bodenheimer, T. (2008). Coordinating care — a perilous journey through the health care system. The New England Journal of Medicine, 358, 1064-1071. doi:10.1056/NEJMhpr0706165.
6. Collins, L. G., & Swartz, K. (2011). Caregiver Care. American Family Physician, 83(11), 1309-1317. Retrieved fromhttps://www.aafp.org/afp/2011/0601/p1309.html
7. Coleman E. A. (2003). Falling through the cracks: challenges and opportunities for improving transitional care for persons with continuous complex care needs. Journal of the American Geriatrics Society, 51,549-555. doi:10.1046/j.1532-5415.2003.51185.x
8. Zweifel, P. (2011). Swiss experiment shows physicians, consumers want significant compensation to embrace coordinated care. Health Affairs, 30(3), 510-518. doi:10.1377/hlthaff.2010.0954
9. Zweifel, P. (2011). Swiss experiment shows physicians, consumers want significant compensation to embrace coordinated care. Health Affairs, 30(3), 510-518. doi:10.1377/hlthaff.2010.0954
10. Dickinson, V. (2015). Docs are leaving behind federal dollars to pay for coordinated care. Modern Healthcare. Retrieved from https://www.modernhealthcare.com/article/20151013/NEWS/151019975
11. https://www.cms.gov
12. https://innovation.cms.gov/initiatives/bundled-payments/
13. https://www.cms.gov
14. Traver, A. (2013). The promise of care coordination: Transforming healthcare delivery. Retrieved fromhttp://familiesusa.org/sites/default/files/product_documents/Care-Coordination.pdf
15. Traver, A. (2013). The promise of care coordination: Transforming healthcare delivery. Retrieved fromhttp://familiesusa.org/sites/default/files/product_documents/Care-Coordination.pdf
16. Conill, A. M., & Horowitz, D.A. (1999). Disease management: Origins, basic principles, and practical considerations. Seminars in Medical Practice, 2(4). Retrieved from http://www.turner-white.com/memberfile.php?PubCode=smp_dec99_dismanorigin.pdf
17. Lipson, D. & Au, M. (2010). Care coordination and disease management. National Governors Association. Retrieved fromhttps://www.mathematica-mpr.com/our-publications-and-findings/publications/care-coordination-and-disease-management
18. Care Coordination. (2015). Agency for Healthcare Research and Quality. Retrieved fromhttps://www.ahrq.gov/ncepcr/care/coordination.html
19. Ehrlich, C., Kendall, E., Muenchberger, H., & Armstrong, K. (2009). Coordinated care: What does that really mean? Health & Social Care In The Community, 17(6), 619-627. doi:10.1111/j.1365-2524.2009.00863.
20. Chen, A., Brown, R., Archibald, N., Aliotta, S., & Fox, P. D. (2000). Best practices in coordinated care. Mathematica Policy Research. Retrieved from https://www.mathematica-mpr.com/our-publications-and-findings/publications/best-practices-in-coordinated-care
21. O’Malley, A. S., Tyan, A., Cohen, G. R., Kemper, N., Davis, W. M. (2009). Coordination of care by primary care practices: Strategies, lessons and implications. Center for Studying Health Care Change. Retrieved fromhttp://www.hschange.org/CONTENT/1058/1058.pdf
22. Conill, A. M., & Horowitz, D.A. (1999). Disease management: Origins, basic principles, and practical considerations. Seminars in Medical Practice, 2(4). Retrieved from http://www.turner-white.com/memberfile.php?PubCode=smp_dec99_dismanorigin.pdf
23. Lipson, D., and M. Au. “Care Coordination and Disease Management.” In “State Roles in Delivery System Reform.” Washington, DC: National Governor’s Association, 2010. Available athttps://www.nga.org/files/live/sites/NGA/files/pdf/1007DELIVERYSYSTEMREFORM.PDF.
24. https://www.ahrq.gov/
25. Oeseburg, B., Wynia, K., Middel, B., Reijneveld, S. A. (2009). Effects of case management for frail older people or those with chronic illness: A systematic review. Nursing Research, 58(3), 201-210. doi:10.1097/NNR.0b013e3181a30941 (http://www.rug.nl/research/portal/files/2690835/Oeseburg_2009_Nurs_Res.pdf).
26. https://nashp.org/
27. https://nashp.org/
28. https://nashp.org/
29. Moss, J. E., Flower, C. L., Houghton M. L., Moss, D. L., Nielsen, D. A., Taylor, D. M., & MacCallum, P. (2002). A multidisciplinary care coordination team improves emergency department discharge planning practice. The Medical Journal of Australia, 177(8), 435-439. Retrieved from https://www.mja.com.au/journal/2002/177/8is
30. Warth, G. J. (2011). Continuity of care starts with you. Medscape Multispecialty. Retrieved fromhttp://www.medscape.com/viewarticle/740856
31. https://www.cms.gov/
32. http://www.nationalpartnership.org/research-library/health-care/HIT/consumer-principles-for-1.pdf
33. https://www.healthit.gov/sites/default/files/onc-beacon-lg2-strengthening-care-mgmt-with-hit.pdf
34. https://www.healthit.gov/sites/default/files/onc-beacon-lg2-strengthening-care-mgmt-with-hit.pdf
35. http://c.ymcdn.com/sites/www.iowapca.org/resource/resmgr/imported/cc%20cm%20cm%20n av%20definitions.pdf
36. https://www.webopedia.com/TERM/S/structured_data.html
37. https://www.webopedia.com/TERM/U/unstructured_data.html
38. https://blog.healthlanguage.com/blog/bid/216980/How-a-Terminology-Server-Can-Support-an-EHR
39. https://blog.healthlanguage.com/blog/bid/216980/How-a-Terminology-Server-Can-Support-an-EHR
40. http://wiki.hl7.org/index.php?title=Case_Management/Disease_Management_C-CDA_R2.x_Project_Documents
41. https://www.himss.org/library/health-information-exchange/FAQ
42. https://www.wisegeek.com/what-is-an-information-repository.htm
43. https://searchmicroservices.techtarget.com/definition/application-program-interface-API
44. Reducing waste in health care. Health Aff, Health Policy Brief. December 13, 2012.
45. USA TODAY analysis of Centers for Medicare & Medicaid Services data, Meghan Hoyer and Frank Pompa.
46. Multiple Chronic Conditions Chartbook. AHRQ Publications No, Q14-0038. Rockville, MD: Agency for Healthcare Research and Quality. April 2014.
47. http://www.rug.nl/research/portal/files/2690835/Oeseburg_2009_Nurs_Res.pdf
48. https://onlinelibrary.wiley.com/doi/full/10.1111/j.1365-2753.2011.01805.x
49. Ostrovsky et al. Submitted.
50. Frost et al. Improving Sickle Cell Transitions of Care Through Health Information Technology. Am J Prev Med 2016;51(1S1):S17–S23.
51. Richardson JE, et al. A needs assessment of health information technology for improving care coordination in three leading patient-centered medical homes. J Am Med Inform Assoc 2015;22:815–820.
52. https://www.sciencedirect.com/science/article/pii/S1532046415000453
53. Posnenkova et al. Active ambulatory care management supported by short message services and mobile phone technology in patients with arterial hypertension. J of Amer Soc of Hypertension. 2012: 6(5). 346-355. Available online at:https://www.researchgate.net/publication/230894319_Active_ambulatory_care_management_supported_by_short_message_services_and_mobile_phone_technology_in_patients_with_arterial_hypertension.
54. Marek KD et al. Nurse care coordination and technology effects on health status of frail older adults via enhanced self-management of medication: randomized clinical trial to test efficacy. Nurs Res. 2013; 62(4): 269–278. Available online at:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3706033/
55. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3814806
56. https://academic.oup.com/jamia/article-abstract/19/3/328/2909132
57. https://www.ncbi.nlm.nih.gov/pubmed/26195588
58. https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/clm104c12.pdf
59. https://www.aafp.org/fpm/2005/0500/p23.html.
60. Chronic Care Management (CCM), CMS-Learning Network. Available online at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/ChronicCareManagement.pdf. Last accessed: 08/8/2016.
61. Pershing, Yoakly and Associates. Providing and Billing Medicare for Chronic Care Management. Available online at:http://us.icw-global.com/newsroom.html?file=files/icw/content/pdfs/Brochures/us/icw-Providing%20and%20Billing%20Medicare%20for%20Chronic%20Care%20Management.pdf. Last accessed: 08/08/2016.
62. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/Transitional-Care-Management-Services-Fact-Sheet-ICN908628.pdf
63. Medicaid Coverage Eligibility, Medicaid. Available online at: http://www.medicaid.gov/Medicaid-CHIP-Program-Information/By-Topics/Eligibility/Eligibility.html. Last accessed 06/22/2013.
64. http://www.chcs.org/media/ICRC_Care_Coordination_FINAL_7_29_13.pdf.
65. PACE Program, Centers for Medicare & Medicaid Services (CMS). Available online at: http://www.medicare.gov/your-medicare-costs/help-paying-costs/pace/pace.html. Last accessed: July, 15 2015.
66. The Importance of Home and Community Based Settings in Population Health Management, Philips White Paper, March 2013. Available online at:https://www.leadingage.org/sites/default/files/The_importance_of_home_and_community_March_2013_1.pdf
67. CMMI Innovations Models and Initiatives, CMMI, CMS. Available online at: http://innovation.cms.gov/initiatives/index.html. Last accessed 06/22/2013.
68. Technology Related Provisions in the ACA, LeadingAge CAST. Available online at:https://www.leadingage.org/sites/default/files/Provisions_Relevant_to_Aging_Services_Technologies_HR_3590.pdf?_ga=2.156245951.521688287.1655814431-1417126119.1652800600
69. Medicare Hospital Readmission Reduction Program, CMS. Available online at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/Readmissions-Reduction-Program.html. Last accessed 06/22/2013.
70. CMS ACO Initiatives, CMMI, CMS. Available online at: http://innovation.cms.gov/initiatives/ACO/. Last accessed 06/22/2013.
71. Retrospective Acute Hospital Stay plus Post-Acute Services Payment Bundling Demonstration, CMMI, CMS. Available online at: http://innovation.cms.gov/initiatives/BPCI-Model-2/. Last accessed 06/22/2013.
72. Retrospective Post-Acute Care Only Payment Bundling Demonstration, CMMI, CMS. Available online at:http://innovation.cms.gov/initiatives/BPCI-Model-3/. Last accessed 06/22/2013.
73. http://www.thescanfoundation.org/sites/default/files/roi_calculator_instructions-the_business_case_and_person-centered_care_june_2016.pdf
74. Chavis V, Lemieux J, and Vuckovic N. Global Imperative to Redesign the Nucleus of Care – An Intel White Paper on Coordinated Primary Care. Santa Clara, CA: The Intel Corporation; June 2012. p. 14.
75. Health Quality Ontario. Quality Monitor – 2012 Report on Ontario’s Health System. Toronto, ON: Queen’s Printer for Ontario, 2012. p. 36.
76. Health Quality Ontario. Best Path, A Resource for Health Links – Evidence Informed Improvement Package, Transitions of Care. Toronto, ON: Queen’s Printer for Ontario, 2013. p. 11.
77. Victorian Government Department of Health. Strengthening assessment and care planning – A guide for HACC assessment services in Victoria. Melbourne, Victoria: Aged Care Branch Victorian Government Department of Health, March 2011. p 147.
78. Mental Health Commission. Guidance Document on Individual Care Planning Mental Health Services. Dublin, Ireland: Mental Health Commission. April 2012. p.10.
79. Meyers D, Peikes D, Genevro J, Peterson Greg, Taylor EF, Tim Lake T, Smith K, Grumbach K. The Roles of Patient-Centered Medical Homes and Accountable Care Organizations in Coordinating Patient Care. AHRQ Publication No. 11-M005-EF. Rockville, MD: Agency for Healthcare Research and Quality. December 2010. p. 4.